Women with endometriosis may have problems getting pregnant, as endometriosis is often associated with female infertility.
Specifically, 30% to 50% of patients with endometriosis will have difficulty becoming mothers naturally. Nevertheless, depending on the degree of endometriosis, assisted reproduction techniques may be the solution to achieve the desired pregnancy.
In addition, pregnancy is beneficial for women with endometriosis, as gestation decreases the symptoms of the disease.
Provided below is an index with the 9 points we are going to expand on in this article.
- 1.
- 2.
- 2.1.
- 2.2.
- 2.3.
- 3.
- 4.
- 5.
- 6.
- 6.1.
- 6.2.
- 6.3.
- 6.4.
- 6.5.
- 6.6.
- 6.7.
- 6.8.
- 7.
- 8.
- 9.
Is it possible to become pregnant with endometriosis?
Having endometriosis does not necessarily mean that there is a sterility problem. In fact, 50-70% of women with endometriosis achieve pregnancy without any complications.

On the other hand, the rest of patients with endometriosis will present infertility derived from the disease, either by tubal obstruction or reduction of the ovarian reserve, among other causes. In these cases, these patients will have to resort to different assisted reproduction techniques to achieve pregnancy. In fact, many patients with endometriosis are unaware that they suffer from this disease and will be diagnosed when they see a specialist for fertility problems.

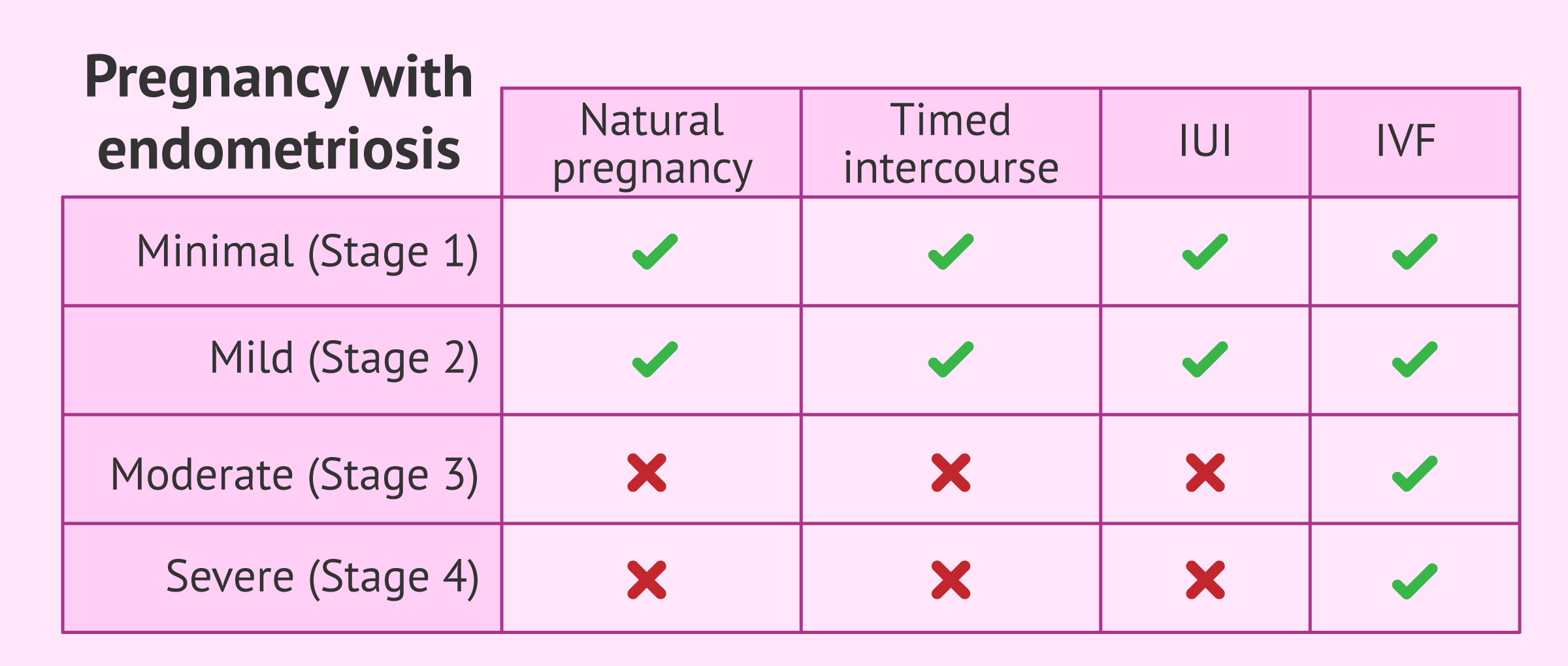
In any case, the difficulty in achieving gestation will depend on the degree and extent of endometriosis by the female reproductive system. Thus, endometriosis has different stages (I to IV) corresponding to minimal, mild, moderate and severe involvement.
Therefore, if the woman knows that she has endometriosis, the first step to take when she wishes to have children is to have a review of the state of the endometriosis. This will allow the patient, with the help of the specialist, to assess the possible options for achieving pregnancy.
Chances of achieving pregnancy
In the following section, we will discuss each of the possible treatments for having children with endometriosis.
Natural Pregnancy
It is true that women with endometriosis may have a more difficult time getting pregnant naturally, but it is not impossible to achieve a natural pregnancy with endometriosis.
The probability of pregnancy each month is 20-25% in women without fertility problems, while in women with endometriosis it is about 2-10%.
In some cases, the gynaecologist may consider it necessary to perform surgery to remove adhesions and endometriotic cysts. The aim is to improve the fertility of these women and increase the pregnancy rate. However, surgery may involve the removal of healthy ovarian tissue and thus lead to impaired fertility. Therefore, this approach is only performed when it is considered appropriate.
To increase the chances of success, the doctor can also monitor the woman's menstrual cycles and control the exact time of ovulation by hormone tests, called directed intercourse.

On the other hand, it is also advisable to avoid negative factors for fertility, such as smoking and obesity.
Artificial insemination or IVF
If a natural pregnancy is not achieved after one year (6 months if the woman is over 35 years old), it will be necessary to go to an assisted reproduction centre for the most appropriate treatment. This period of time may also vary depending on the progression of the disease.
If you need to undergo IVF to become a mother, we recommend that you generate your Fertility Report now. In 3 simple steps, it will show you a list of clinics that fit your preferences and meet our strict quality criteria. Moreover, you will receive a report via email with useful tips to visit a fertility clinic for the first time.
In particular, the technique used will depend on several factors, especially the degree of severity of endometriosis. These are discussed below:
- Artificial insemination
- for young patients with endometriosis type I and II with permeable tubes who have not achieved natural pregnancy within one year. It is also necessary for the men to have good sperm quality.
- In vitro fertilization (IVF)
- either conventional IVF or ICSI would be indicated for patients with moderate or severe endometriosis (grades 3 or 4). It is also the right choice when the artificial insemination was not successfull.
As in the previous section, the specialist may recommend laparoscopy before beginning fertility treatment to improve the likelihood of pregnancy.
However, other specialists believe that surgery can damage healthy tissue during surgery and cause further deterioration of fertility.
In short, it is necessary to assess each case in a personalized way to make the decisions that result in the greatest possible benefit for patients.
Egg donation
Sometimes, in the most serious cases of endometriosis or when previous treatments have failed, the last option left to become mothers is egg donation.
As a matter of fact, 10% of recipients of donor eggs are patients with endometriosis.
In the next section we are going to discuss cases in which donor eggs greatly favor endometriosis patients:
- The degree of endometriosis is very severe
- Ovarian reserve is low
- Oocyte quality is very poor
- Access to the ovaries for ovarian puncture is impossible due to the presence of endometrial tissues.
- The possibility of obtaining eggs is very low because there has been an intervention that has affected the ovarian tissue
Donor eggs have a higher rate of fertilization. The embryos obtained also have better morphology and development than the embryos of women with endometriosis.

Since endometriosis is a progressive disease that affects a woman's fertility, it would be advisable to vitrify the eggs to preserve fertility when being diagnosed mild or moderate endometriosis.
This allows the patient to achieve pregnancy at a later stage, even though the endometriosis has progressed and affected the ovaries. You can read more about it here: Donor-Egg IVF Procedure for Recipients - Protocol & Cost.
Fertility preservation
Because endometriosis is a disease that progressively advances, it can increasingly affect a woman's fertility. This is why fertility preservation is also an option to avoid certain problems in achieving pregnancy with endometriosis.
In principle, the ideal would be to vitrify the eggs to preserve fertility at the time of diagnosis of mild or moderate endometriosis (if the patient is not seeking pregnancy at that time). This would allow the woman to achieve pregnancy at a later stage, even if the endometriosis has progressed and affected the ovaries more.

You can read more about fertility preservation here: Fertility Preservation - Cost & Options for Retaining Your Fertility.
Pregnancy Risks
Some studies in patients with endometriosis seem to indicate that there is a greater likelihood of complications associated with pregnancy.
Structural and functional changes in the female reproductive system due to endometriosis may affect the development of the placenta, so pregnancy may be compromised in these women.
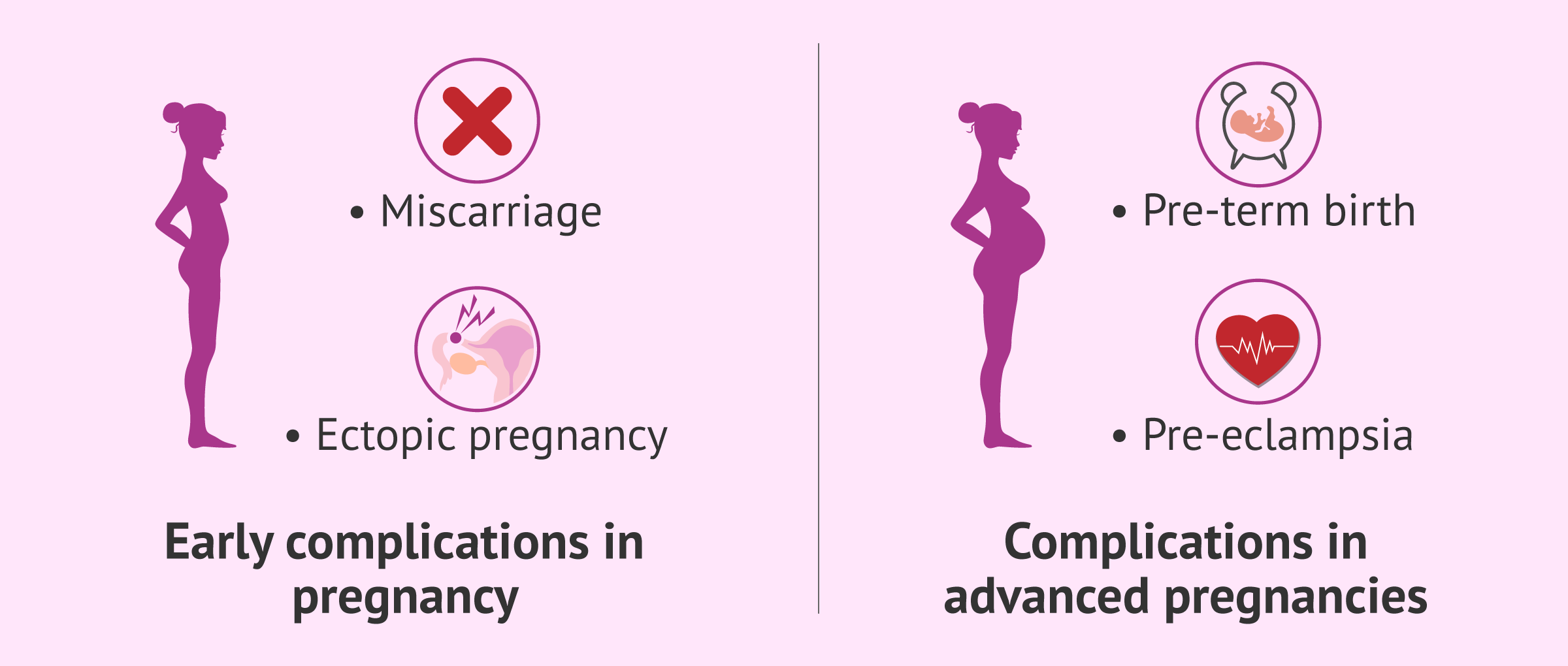
In addition to this, the risks that may appear throughout gestation in patients with endometriosis are the following:
- Miscarriage
- loss of gestation before the 20th week. Women with endometriosis have a 76% higher risk of miscarriage than other women.
- Ectopic Pregnancy
- implantation of the embryo outside the uterus. The probability is 3 times higher in women with endometriosis.
- Preeclampsia
- high blood pressure that usually manifests in the second or third trimester of pregnancy.
- Alterations in delivery
- women with endometriosis are at increased risk of preterm birth or cesarean delivery.
For all these reasons, although pregnancies in women with endometriosis are not considered to be of high risk, they should be more watched and cared for to prevent any type of problem that may affect the fetus or the mother.
Pregnancy improves endometriosis
During pregnancy, a woman's menstrual cycle stops because there is no secretion of female hormones that regulate ovulation and menstruation.
The ovaries are kept at rest and, therefore, there is no production of estrogen, the hormones that promote the growth and development of endometrial plaques.
Pregnancy thus has a protective effect on the development of the disease. During gestation, the patient will notice an improvement in symptoms such as pain.
However, it is important to bear in mind that pregnancy is not the solution for endometriosis, as it will reappear once a woman has given birth and menstrual cycles return.
Gestation is only a transient improvement of endometriosis and not the definitive cure.
FAQs from users
What is the best treatment option to cure endometriosis and be able to get pregnant?
Endometriosis is a chronic condition and there is no cure. Surgery to excise and/or ablate endometriosis can increase the chance of pregnancy, but repeat surgeries are not successful. The treatment of choice depending on the age of the woman and the extent of the endometriosis includes ovulation induction with IUI’s and IVF. IVF is more successful but is also more costly and is not as available.
What are your reproductive options if you have stage IV endometriosis?
Endometriosis affects 10-15% of all women. Of women with endometriosis, 30-50% are estimated to have infertility; of women with infertility, 25-50% are estimated to have severe endometriosis. A hallmark of endometriosis is inflammation and subsequent formation of adhesions in the pelvis. These adhesions distort the pelvic anatomy and impacts the woman in a variety of ways. The most direct consequence of adhesions can be a disruption of the anatomical relationship between the ovaries and fallopian tubes. In advanced cases of endometriosis, tubal blockage may occur to the point of a hydrosalpinx which may require removal before any fertility treatment.
The most appropriate treatment for each couple will depend on a number of factors including the woman’s age, the duration of infertility, her ovarian reserve, the sperm analysis, a history of past surgery for endometriosis and its severity.
For women younger 35 years of age with low stage disease, a trial of Fertility treatment with intrauterine insemination (IUI) is recommended. However, for women greater than or equal to 35 years of age with advanced stages of endometriosis (stages III and IV), IVF is recommended due to the higher pregnancy rate. Of note, advanced endometriosis, compared to other diagnoses, may reduce the pregnancy rate with in vitro fertilization.
Which is more effective with mild endometriosis, IUI or IVF?
Intrauterine Insemination (IUI) is the treatment of choice for young patients with mild-to-moderate endometriosis (stages I and II). For this treatment to be possible, no blockage in the Fallopian tubes must exist. However, recent studies suggest that IUI may be ineffective in these cases. The latest European review on the average success rates during years 2016-2017 with AIH (artificial insemination by husband) are below 15% per cycle. So, in conclusion, opting for IUI in cases of mild-to-moderate endometriosis is possible in very particular cases where there is evidence that it might work.
In general, In Vitro Fertilization (IVF) is the first option for patients with a moderate or severe type of endometriosis (stages III and IV), as well as for women with previous failed cycles in spite of having a good prognosis initially.
Can you get pregnant with endometriosis without surgery?
Unfortunately, the chances are very low. While painkillers or hormonal treatments can help relieve the symptoms of endometriosis, laparoscopic surgery is necessary to achieve pregnancy with endometriosis, even in mild-to-moderate cases.
Can you get pregnant with untreated endometriosis?
As explained earlier, it is highly unlikely. Endometriosis should be properly managed by means of laparoscopic surgery.
What are the chances of getting pregnant with one tube and endometriosis?
The odds of falling pregnant with one Fallopian tube should not be different than any other woman as long as the remaining tube is working normally. Depending on the stage of endometriosis, you may need IVF to get pregnant.
What are the dangers of being pregnant with endometriosis?
Several studies have indicated that endometriosis is a risk factor for complications during pregnancy. Your doctor should advise you on the potential risks associated according to the severity of your endometriosis.
The risks associated with pregnancy in women with endometriosis include increased risk of miscarriage, ectopic pregnancy, placenta displacement, spontaneous rupture of the uterus, obstructed labor, postpartum hemorrhage, and preterm birth.
How does pregnancy help endometriosis?
No, pregnancy does not cure endometriosis. Although it is a widespread myth, it is actually true that pregnancy may temporarily suppress the symptoms of endometriosis. However, this does not mean that it eradicates the disease itself.
Suggested for you
The ovarian reserve can be affected as a result of endometriosis in the ovary. To find out how this affects a woman's fertility, click here: How many eggs does a woman have?
We have talked about the preservation of fertility as a method to avoid the deterioration of the oocyte quality. If you want to know what this method consists of, read on here: Fertility preservation- cost & options for retaining your fertility.
We make a great effort to provide you with the highest quality information.
🙏 Please share this article if you liked it. 💜💜 You help us continue!
References
ADAEC. Endometriosis: Documento de consenso S.E.G.O. La voz digital [periódico digital] 2007.
Adamson GD, et al. Creating solutions in endometriosis: global collaboration through the World Endometriosis Research Foundation. J of Endometriosis 2010;2(1):3-6.
Allen C, Hopewell S, Prentice A. Non-steroidal anti-inflammatory drugs for pain in women with endometriosis. Cochrane Database of Systematic Reviews 2005, Issue 4.
American College of Obstetricians and Gynecologists (ACOG). Medical management of endometriosis. Washington (DC): American College of Obstetricians and Gynecologists (ACOG); 1999 Dec. 14 p. (ACOG practice bulletin; no. 11).
ASRM American Society for Reproductive Medicine. Endometriosis. Guía para pacientes. En: Serie de Información para pacientes. Revisado en 2013. Birmingham, Alabama.
Clement PB. The pathology of endometriosis: a survey of the many faces of a common disease emphasizing diagnostic pitfalls and unusual and newly appreciated aspects. Adv Anat Pathol. 2007; 14(4):241-60
Davis L, Kennedy SS, Moore J, Prentice A. Modern combined oral contraceptives for pain associated with endometriosis. Cochrane Database of Systematic Reviews: Reviews 2007, Issue 3.
Di W, Guo SW. Curr Opin Obstet Gynecol. The search for genetic variants predisposing women to endometriosis. 2007; 19(4):395-401.
Dra. MA. Martínez Zamora. (2013). Actualización sobre la etiopatogenia de la endometriosis. Hospital Clínic Universitari de Barcelona. Acadèmia de Ciències Mèdiques i de la Salut de Catalunya i de Balears, Societat Catalana d’Obstetricia i Ginecologia
European Society for Human reproduction (ESHRE). Guideline for the diagnosis and treatment of endometriosis. Human Reproduction, 2005; 20(10):2698-2704.
Giudice LC. Endometriosis. Clinical Practice. N Engl J Med 2010;362(25):2389-98.
Guo S-W, et al. Reassessing the evidence for the link between dioxin and endometriosis: from molecular biology to clinical epidemiology. Mol Hum Reprod 2009;15(10):609-24.
Hughes E, Fedorkow D, Collins J, Vandekerckhove P. Ovulation suppression for endometriosis. Cochrane Database of Systematic Reviews 2003, Issue 3.
Husby GK1, Haugen RS, Moen MH. Diagnostic delay in women with pain and endometriosis. Acta Obstet Gynecol Scand. 2003 Jul;82(7):649-53.
Marcoux S., Maheux R., Berube S (1987). Laparoscopic surgery in infertile women with minimal or mild endometriosis. Canadian Collaborative Group on Endometriosis. New England Journal of Medicine; 337: 217-22.
Nnoaham KE, et al. Impact of endometriosis on quality of life and work productivity: a multicenter study across ten countries. Fertil Steril 2011;96(2):366-373.
Reproducción Asistida ORG. Video: ¿La ovodonación ofrece buenos resultados en pacientes con endometriosis?
(Is egg donation a good option in patients with endometriosis?), by Blanca Paraíso, MD, PhD, MSc, Dec 19, 2017. .
Rogers PA, et al. Priorities for endometriosis research: recommendations from an international consensus workshop. Reprod Sci 2009;16(4):335-46.; Adamson GD, et al. Creating solutions in endometriosis: global collaboration through the World Endometriosis Research Foundation. J of Endometriosis 2010;2(1):3-6.
Royal College of Obstetricians and Gynaecologists. The investigation and management of endometriosis. London: RCOG; 2006. Green-top Guideline No. 24.
Simoens S, Hummelshoj L, D'Hooghe T. Endometriosis: cost estimates and methodological perspective. Hum Reprod Update. 2007; 13(4):395-404.
Society of Obstetricians and Gynaecologists of Canada. Consensus guidelines for the management of chronic pelvic pain. Ottawa: SOGC; 2005. SOGC Clinical Practice Guidelines No 164.
Vigano P, et al. The relationship of endometriosis and ovarian malignancy: a review. Fertil Steril 2008;90(5):1559-70.
Vigano P, Somigliana E, Vignali M, Busacca M, Blasio AM. Genetics of endometriosis: current status and prospects. Front Biosci. 2007; 12:3247-55.
Wieser F, Cohen M, Gaeddert A, Yu J, Burks-Wicks C, Berga SL, Taylor RN. Evolution of medical treatment for endometriosis: back to the roots? Hum Reprod Update. 2007; 13(5):487-99.
FAQs from users: 'What is the best treatment option to cure endometriosis and be able to get pregnant?', 'What are your reproductive options if you have stage IV endometriosis?', 'Which is more effective with mild endometriosis, IUI or IVF?', 'Can you get pregnant with endometriosis without surgery?', 'Can you get pregnant with untreated endometriosis?', 'What are the chances of getting pregnant with one tube and endometriosis?', 'What are the dangers of being pregnant with endometriosis?' and 'How does pregnancy help endometriosis?'.






Hi!
I’m an endometriosis patient and currently considering getting pregnant. I tried to conceive naturally and it didn’t work out. So I’m looking for a fertility clinic in my area (NY) that specializes in treating endometriosis patients. I’d love to hear some suggestions, please.
I’d also like to know which fertility treatment is best in my case.
Thank you so much,
yours Suzy
Hi Suzy,
I’m so sorry to hear this. Endometriosis patients usually have trouble getting pregnant naturally.
Your treatment of choice would be in vitro fertilization. If you want to learn what this technique is about, I suggest you the following article: What is In Vitro Fertilization (IVF)?
As for fertility clinics, I recommend you fill in our fertility report. You’ll receive a list of suitable fertility clinic near your which best fits your needs.
Hope this helps,
wish you all the best!