IVF is the medical abbreviation for in vitro fertilization, a challenging Assisted Reproductive Technology (ART) from the technical viewpoint that is used to help couples or women who have trouble conceiving.
The success rates of IVF depend on multiple factors, but undoubtedly age is a key factor. Also, the quality of the sperm used plays a major role when it comes to determining the chances of getting pregnant with IVF.
The total cost of in vitro fertilization procedures is considerably high due to two main aspects: on the one hand, the hormonal medications used to induce ovulation, and on the other hand, the varied range of modern technologies and lab equipment used.
The different sections of this article have been assembled into the following table of contents.
In vitro fertilization is an Assisted Reproductive Technology (ART) that involves the collection of eggs from the woman's ovaries by means of follicle puncture (ovum pick-up). Then, they are fertilized at the laboratory using the husband's or partner's sperms. The development of the resulting embryos is monitored until the embryo or embryos selected are transferred back to the woman's uterus. The ultimate goal is to achieve a healthy pregnancy.

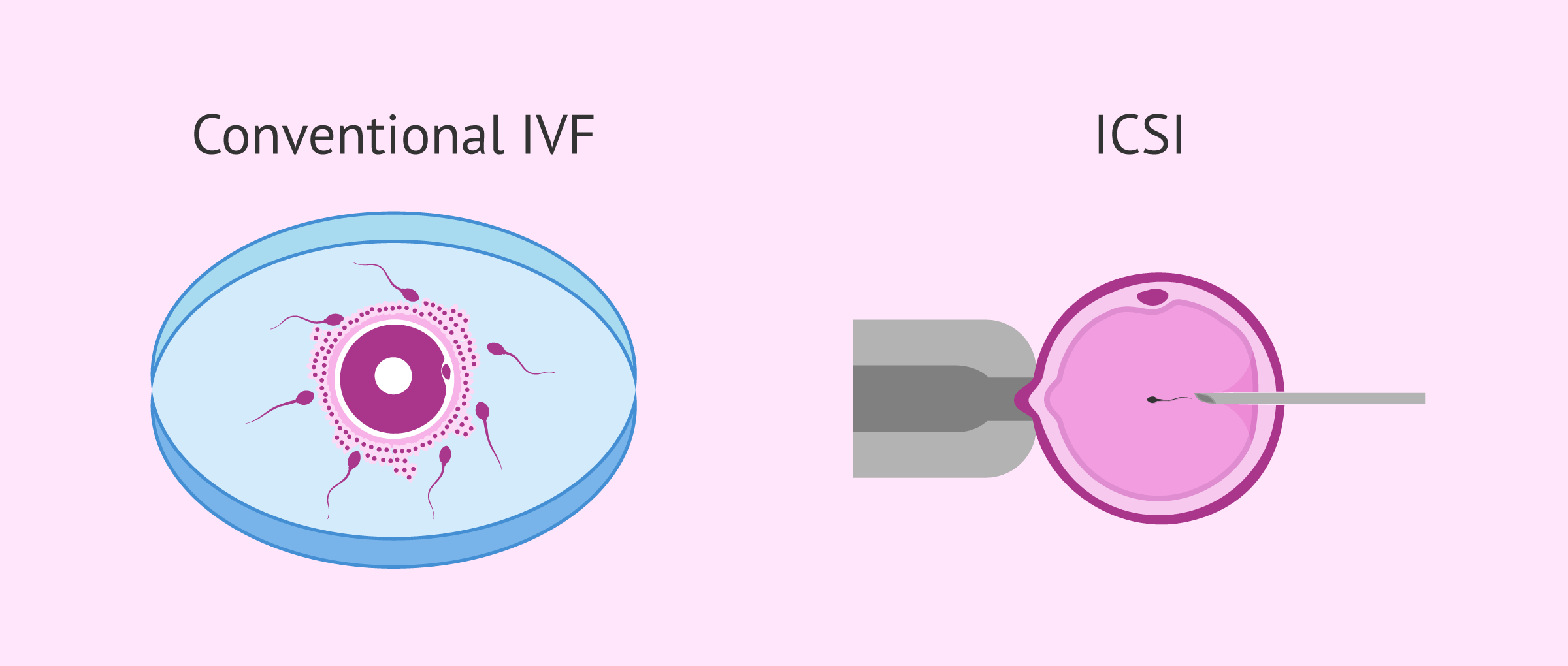
Depending on how the egg and the sperm cell are fused together, we can distinguish between two types of IVF:
Choosing between the former or the latter depends on what is causing female and/or male infertility in the couple, as well as the particularities of each fertility clinic. Still, even though the fertilization process varies, the previous steps are the same.
If you want to know more details about the differences between one and the other way of gamete fusion, you can read this article: IVF or ICSI: What is the difference? Which is better?
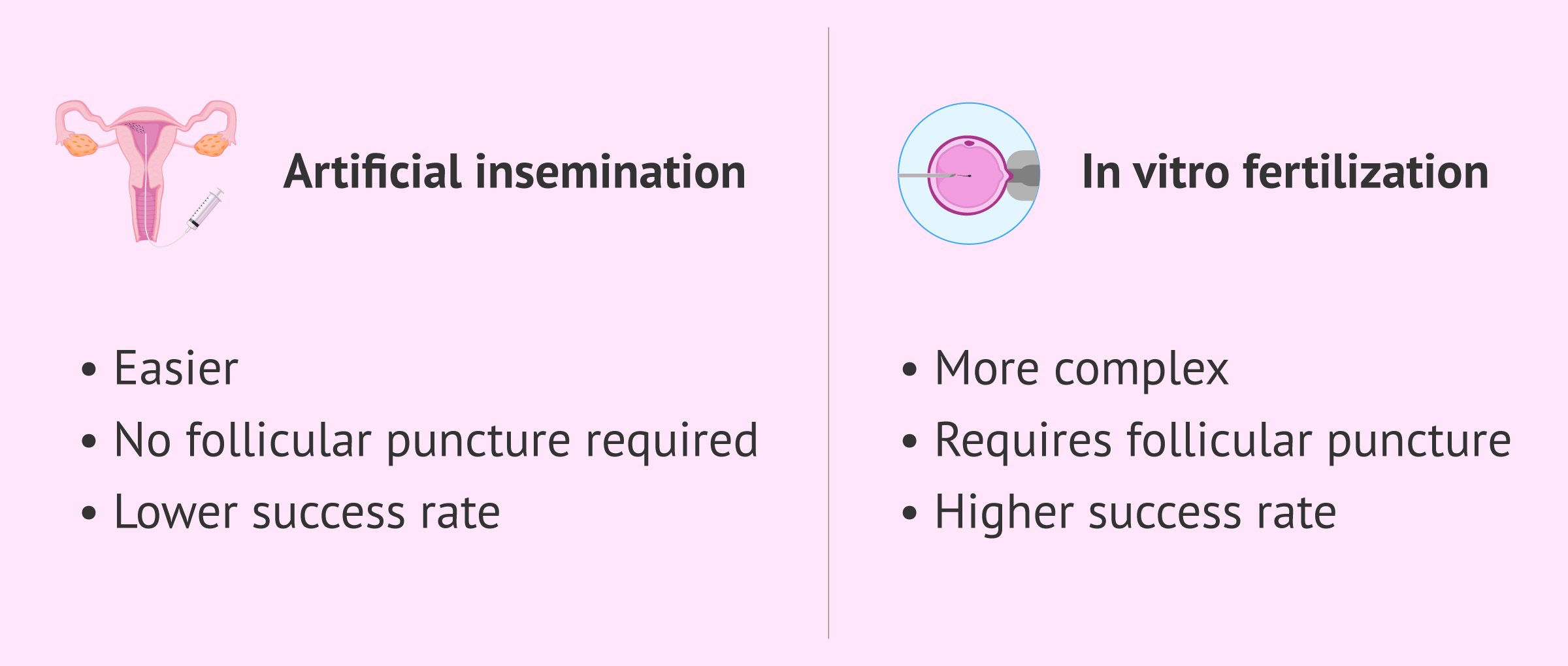
Artificial insemination (AI), better known as intrauterine insemination or just IUI, is another infertility treatment, though less technically challenging than IVF. With IUI, the partner's sperm is inserted into the female's uterus, and fertilization occurs inside the female reproductive tract as it would with sexual intercourse, without further medical involvement.
So, as one shall see, IVF involves a higher degree of complexity than artificial insemination (AI)—not only the number of steps to follow is higher, but also the involvement of the specialist. In fact, IVF requires a simple surgical procedure to retrieve the eggs, while with IUI this step is unnecessary.
Its success rates, however, are higher, and this is the reason why it is the treatment of choice in the majority of the cases.
You may hear terms such as in vitro insemination, which actually is incorrect as you may have understood with the definition of each technique given above.
The following post contains further info on this topic: Artificial insemination vs. in vitro fertilization.
A couple may need IVF treatment to have a baby due to a wide range of causes. Male infertility, female infertility or both may be the reason why this infertility treatment is recommended.
The following are the most common indications of in vitro fertilization:
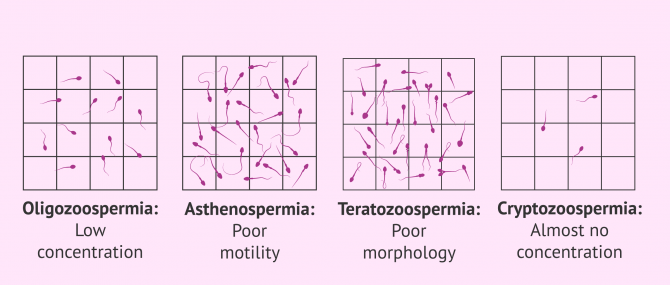
Moderate-to-severe cases of male infertility can be treated by means of IVF:
If you are interested in further reading about this topic, we recommend you read the following article: What Causes Male Infertility? - Symptoms & Treatment.
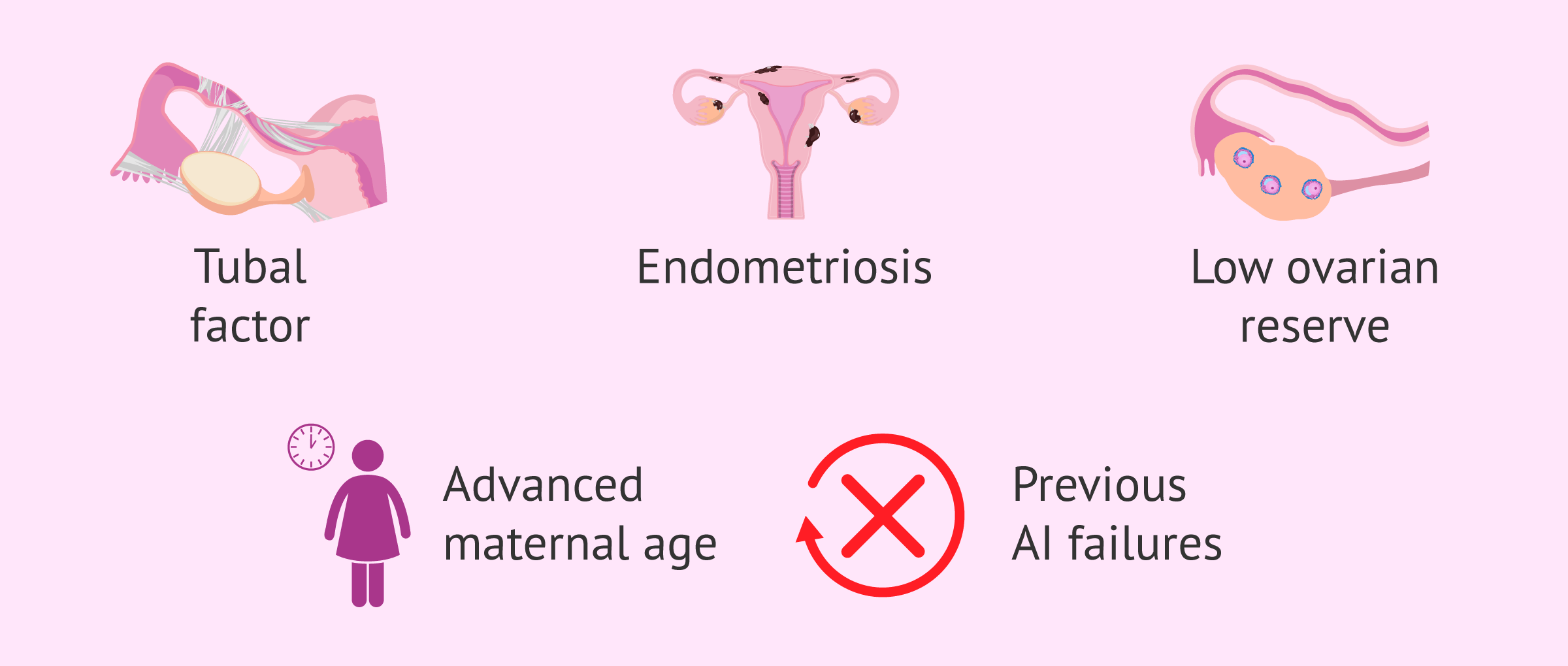
In the case of women, fertility problems are often linked to the following factors:
In addition, IVF would also be indicated in case of previous failures in artificial insemination (IUI).
Although the in vitro fertilization technique is a widespread technique that can help many patients, the truth is that it has some requirements.
In order to perform in vitro fertilization, it is necessary that the woman is able to produce mature eggs. In addition, it is necessary that the patient does not have uterine problems or anomalies that prevent the implantation of the embryo or the evolution of the gestation.
On the other hand, if the woman has a diminished ovarian reserve and it is not possible to obtain mature eggs, IVF with donor eggs can be performed. If you want to know what this treatment consists of, you can read the following post: What is ovodonation, and what is the price of the treatment?
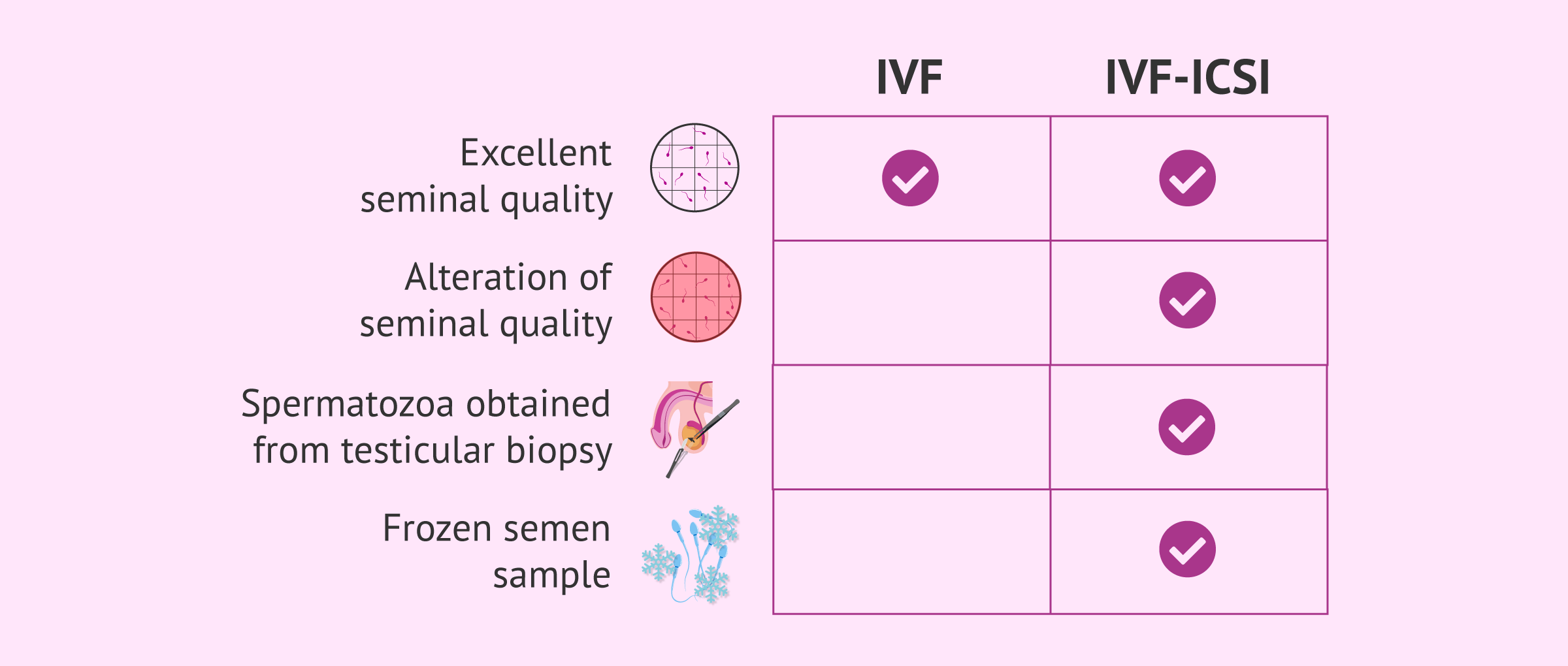
In the case of the male, the requirements vary depending on the type of IVF to be performed. If the seminal quality allows it, conventional IVF can be performed. If, on the other hand, the sperm has serious motility, morphology, or concentration problems, the ICSI technique will be chosen.
In any case, even if the requirements for conventional IVF are met, there are fertility clinics that prefer to perform ICSI.
On the other hand, when semen samples do not come from ejaculate, as in the case of a testicular biopsy, ICSI is also required, since their quality is usually very low. The same can occur when frozen semen is used, since performing an ICSI allows optimizing the amount of cryopreserved sample.
It is also possible to perform IVF with donor sperm in cases of azoospermia or absence of a male partner, and even IVF with double donation, that is, with donated eggs and sperm.
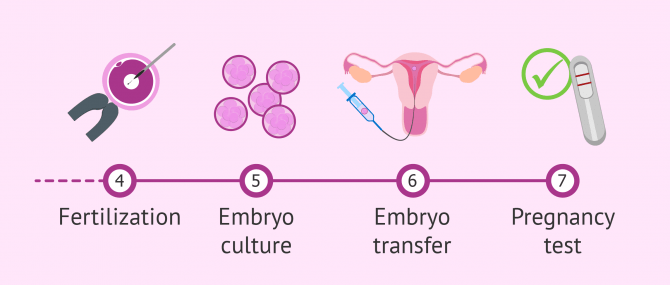
The IVF process can become a tough one for many patients, as they have to go through various steps before achieving success.
The following article explains each of these IVF steps in more detail: What is the IVF process step-by-step like?
Just like other assisted reproductive technologies, IVF success rates are based on several factors, being the patient's age one of the most influential ones.
Experts have been able to establish a series of patterns to grade the odds for success in each case. Such percentages are:
When talking about and comparing the success rates of different techniques or fertility clinics, one should pay attention to the meaning of success in each case. Sometimes, statistical data refers to different percentages, e.g. pregnancy rate, birth rate, live birth rate, etc.
Real IVF outcomes should be based on the live birth rates obtained with this method, and not only on the pregnancy success rate. It should be taken into account that not all pregnancies are successful.
If you want to learn more about IVF success rates and outcomes, the following article may be of interest: Success Rates of IVF.
Like any other infertility treatment (e.g. intrauterine insemination or IUI), in vitro fertilization procedures have a series of advantages and disadvantages. You can find them explained below.
The following are the main advantages of in vitro fertilization:
If you are interested in learning more about this topic, you can continue reading here: What are some of the main advantages of in vitro fertilization?
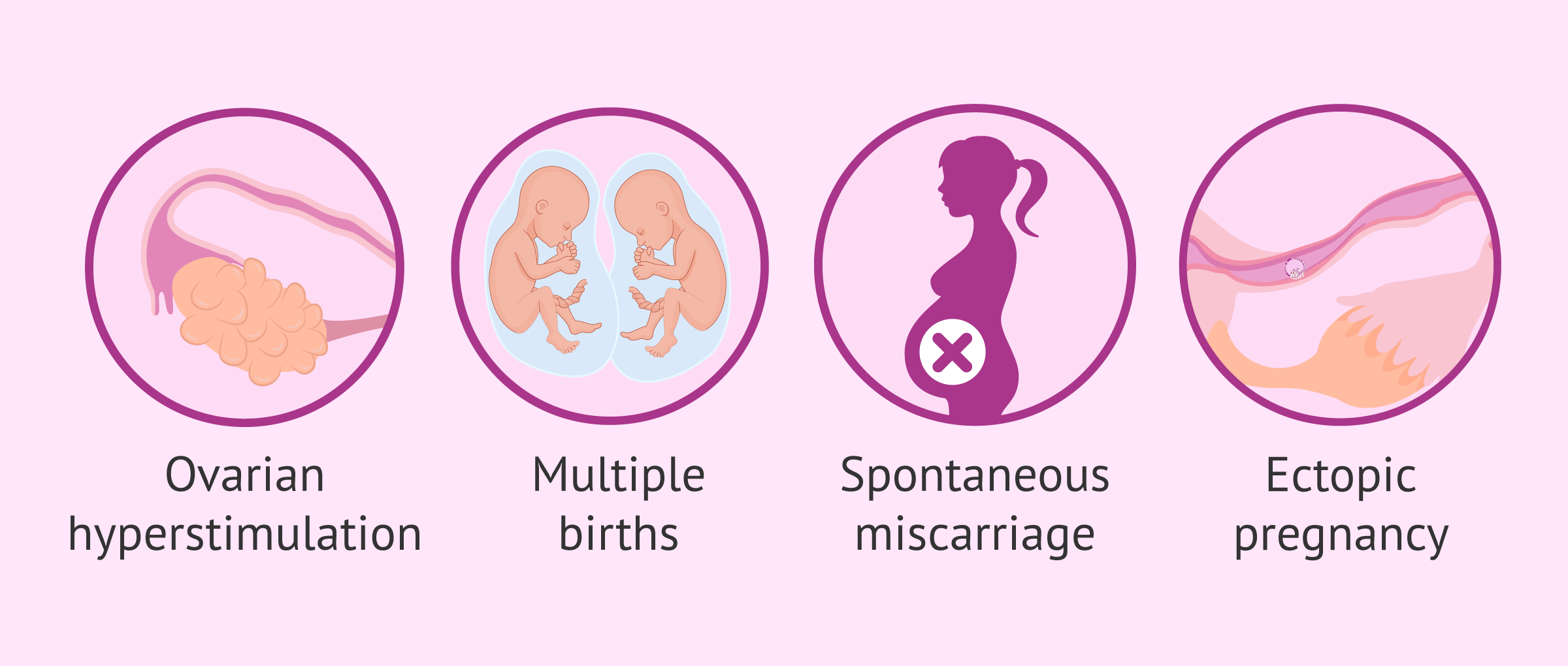
However, IVF carries a series of disadvantages as well:
Regardless of whether you go for a classical IVF cycle or an ICSI, the drawbacks associated are similar.
As seen earlier, ovarian stimulation and follicle puncture can cause a series of adverse reactions. Patients should be informed about all these potential risks before getting started with the treatment.
If you want more information about the risks of IVF, we recommend that you read this article: Side effects of IVF.
Before giving you particular sums, it is important to remark that there are many variables specific to your particular medical case that can influence the overall cost of IVF.
In countries like Spain or the UK, where IVF and other treatments can be covered by the public health system as long as the patient meets a series of requirements, IVF is available for everyone.
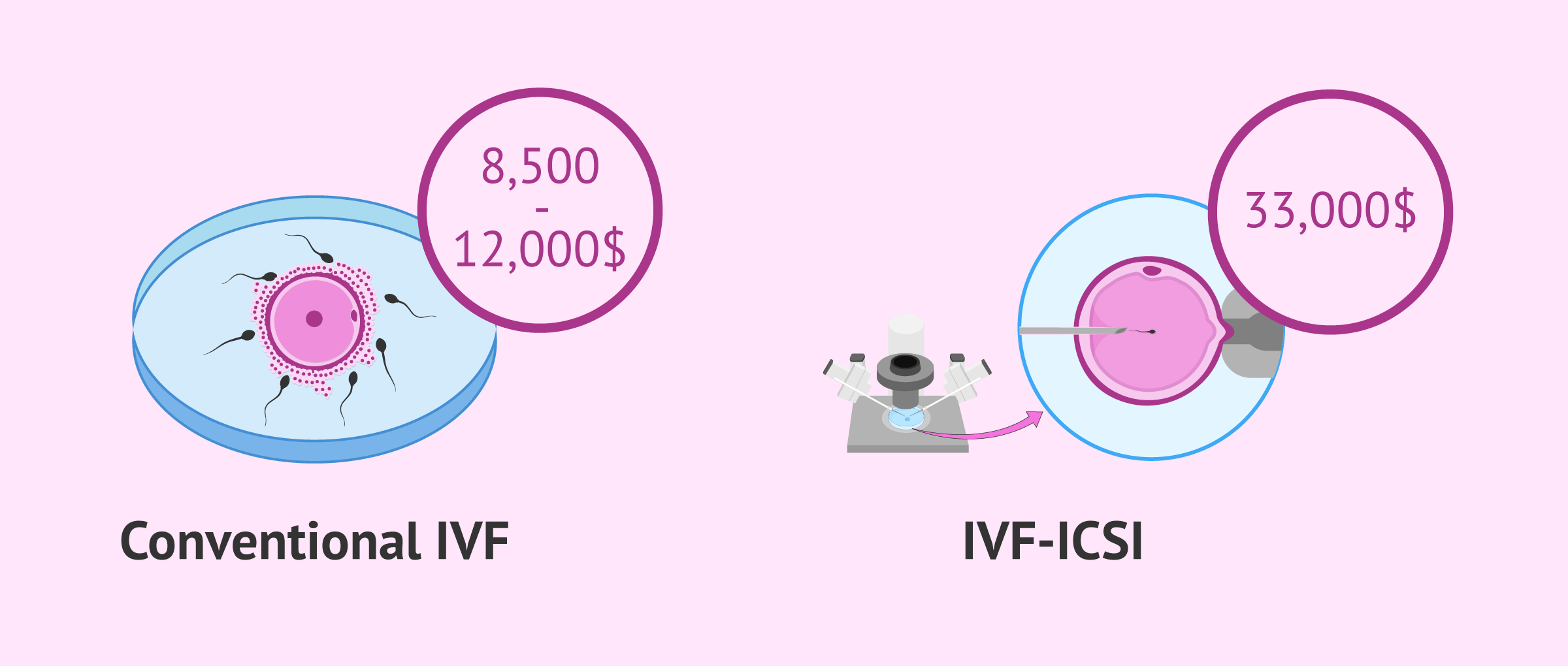
Many US clinics offer different in vitro fertilization cost plans, including multiple cycle packages with different pricing options. For example, single cycle IVF packages using own eggs can range from $8,500 to $12,000.
On the other hand, some fertility clinics offer money-back guarantee programs, available for a higher fee. For example, while a multiple cycle IVF cost plan without money-back guarantee can cost about $16,000, the price with money-back guarantee (usually up to 80%) is typically $18,000 or more.
The availability of these plans is subject to the health insurance plan of each patient. In some IVF centers, multiple cycle IVF cost plans are available only in case the patient is not covered by insurance. However, the standard type of IVF arrangement across the country is a single cycle.
The use of additional techniques contributes to increasing the cost. For example, if ICSI and assisted hatching were necessary, the cost can be as high as $33,000 or over, and using ICSI with PGD for a blastocyst embryo transfer using donor eggs and a surrogate can start from $80,000.
Check out this post to learn more about the costs of surrogacy with egg donation and other fertility treatments involving third parties: Guide to Third Party Reproduction.
If you need to undergo IVF to become a mother, we recommend that you generate your Fertility Report now. In 3 simple steps, it will show you a list of clinics that fit your preferences and meet our strict quality criteria. Moreover, you will receive a report via email with useful tips to visit a fertility clinic for the first time.
The costs of IVF vary on a case-by-case basis, and some women may be eligible to have NHS-funded IVF, provided that they meet the criteria that can be found on the fertility guidelines published by the National Institute for Health and Care Excellence (NICE).
If you decide to have IVF treatment at a private clinic, are not eligible for NHS treatment, or want to skip long waiting lists, the cost of a single IVF cycle can be £5,000 or more.
In the case of women aged under 40 years who have not been able to conceive after 2 years of regular unprotected intercourse or 12 artificial insemination cycles (with 6 or more being by IUI), the NHS will offer them 3 full cycles with or without ICSI.
As for women aged 40-42 years who have not been able to conceive after 2 years of regular unprotected intercourse or 12 cycles of artificial insemination (with 6 or more being by IUI), the NHS will offer them 1 full cycle, with or without ICSI, as long as they meet these requirements:
Also, in cases of unexplained infertility, that is, where evidence shows that there is no chance of pregnancy and IVF is clearly the only effective treatment, your doctor will refer you directly to NHS-funded IVF treatment.
Another possibility for British patients in need of IVF is pursuing this treatment abroad. Often, women who opt for this alternative are in need of egg donation. However, you should keep in mind that the HFEA only licensed clinics in the UK.
The general cost of in vitro fertilization (IVF) in Canada usually starts from $7,000 (Canadian dollars). However, the total cost is expected to be higher, especially if you are not covered by insurance. To the basic cost of IVF treatment, you should add:
It should be noted that the province of Ontario pays for fertility treatments, provided that you are an Ontario resident and have a valid OHIP card. To qualify for Ontario’s Fertility Program (one-time cycle per lifetime of IVF), the woman must be under the age of 43. You can qualify for an additional cycle if you act as a surrogate.
Sometimes pregnancy is not achieved with the first transfer. If there are vitrified embryos, a second transfer can be performed.
If there are no vitrified embryos from the first follicular aspiration, a second IVF cycle can be performed with the advantage of being able to take into account all the information provided by the first cycle. This information is usually very valuable for deciding on actions such as changes in the ovarian stimulation pattern, measures to improve embryo transfer, such as performing a hysteroscopy, and even the possibility of performing a laparoscopy, which can help diagnose hidden pathology such as endometriosis.

It is very important the attitude that is taken before a negative first cycle of assisted reproduction. Being aware that success often does not come the first time can lessen the sadness in the face of a negative result. Specialized psychological support has shown advantages in subsequent cycles.
Medications used in assisted reproduction can produce various side effects such as headaches, mood swings, abdominal pain, hot flashes and bloating. Occasionally, they can cause ovarian hyperstimulation syndrome.

With ovarian stimulation, more eggs are developed than in a natural cycle, but this will not lead to an earlier menopause. Women are born with a finite number of eggs and maturation has no effect and will not bring an earlier end to the reproductive stage.
Pregnancies achieved with fertility treatments have no greater risk of complications than any other.
The precautions are no different from those of any pregnant woman, including the continuation of sexual activity. Once the embryo has implanted, the risks of a pregnancy achieved through IVF are no different than any other. In addition, the recommendations and special care will be more related to the woman's age, in cases of advanced age, and/or history of previous pathologies.
On the one hand, lesbian couples have the chance to have a child through lesbian IVF or intra-partner egg sharing. It is a way for both of them to participate in the process actively, as one becomes the biological mother and the other the birth mother.
Intrauterine insemination (IUI) with donor sperm is another option available for lesbian couples. However, it depends on the chances for conception this treatment may bring to the couple, so fertility tests will be performed prior to choosing between one option or another.
On the other hand, gay men can build their family thanks to surrogacy with donor eggs. In this case, a gestational carrier undergoes IVF with the eggs of another woman, who acts as the egg donor for the intended parents, while one of them delivers the semen sample. Thus, the child will be genetically linked to one of the parents.
Many couples achieve a natural pregnancy after having had an "test tube" baby. It happens in cases where the cause of infertility declines or disappears.
Stress is a good example. Some patients see their fertilizing potential reduced because of the stress caused when trying to conceive. Anxiety can affect egg and sperm quality, thereby hindering the odds of conception.
Making lifestyle changes (relaxing, changing dietary habits, diminishing or stopping the consumption of toxic substances, etc.) can help improve the chances of getting pregnant to a large extent.
Also, it may occur in cases of unexplained infertility.
When IVF is successful, there is no reason why pregnancy symptoms should be different to those of a natural pregnancy. Still, drugs to induce ovulation may cause some side effects such as bloating or nuisance, but in principle they are not expected to be different.
No, it is not normally needed, either after follicle puncture or after the embryo transfer. Bed rest for IVF recovery is recommended only in exceptional cases.
Depending on the cause of the failure of the first IVF attempt, a second attempt may or may not improve the probability of success.
For example, if the failure of the first IVF was due to poor endometrial preparation, the second attempt will change the medication protocol to try to improve this aspect.
Normally, in the second attempt some guidelines are changed to improve the treatment and this usually results in a greater probability of success, although as we have mentioned, it will depend on each situation.
No treatment is better than the other, as both of them have their pros and cons. Depending on the characteristics of each couple and the origin of their fertility problems, IVF or ICSI would be more advisable.
For example, the most severe cases of asthenozoospermia should be treated with ICSI to guarantee a minimum number of chances for success. On the other hand, when the woman suffers from problems with ovulating or blocked fallopian tubes, conventional IVF can help solve the problem successfully.
Conventional IVF is more similar to natural conception and requires a higher degree of gamete manipulation. However, ICSI helps patients make a step forward toward pregnancy, as the egg-sperm binding is done manually.
Following IVF embryo transfer, the next phase of the treatment is known as two-week wait or 2WW, which is defined as the time period between the transfer and the moment when you finally test for pregnancy. If you want to learn more and get some useful tips to survive it, check out this post: What is the Two-Week Wait (2WW)? – Tips to Survive It.
Also, if you are interested in learning more about ICSI, a more challenging type of IVF, we recommend that you visit this post: What Is ICSI or Intracytoplasmic Sperm Injection?
We make a great effort to provide you with the highest quality information.
🙏 Please share this article if you liked it. 💜💜 You help us continue!
Alper M, Brinsden PR, Fischer R, Wikland M (2002). Is your IVF program good? Hum Reprod; 17: 8-10 (View)
Andersen AN, Gianaroli L, Felberbaum R, de Mouzon J, Nygren KG (2005). Assisted reproductive technology in Europe, 2001. Results generated from European registers by ESHRE. Hum Reprod; 20: 1158 – 1176 (View)
Andersen AN, Goossens V, Ferraretti AP, Bhattacharya S, Felberbaum R, de Mouzon J, Nygren KG, The European IVF-monitoring (EIM) Consortium, for the European Society of Human Reproduction Embryology (ESHRE) (2008). Assisted reproductive technology in Europe, 2004: results generated from European registers by ESHRE. Hum Reprod; 23: 756 – 771 (View)
ASRM, American Society for Reproductive Medicine (2002). Revised minimum standards for in vitro fertilization, gamete intrafallopian transfer, and related procedures. A Practice Committee Report. Guidelines and Minimum Standards (View)
Aytoz A., Camus M., Tournaye H., Bonduelle M., Van Steirteghem A. and Devroey P. (1998): Outcome of pregnancies after intracytoplasmic sperm injection and the effect of sperm origin and quality on this outcome. Fertil. Steril. 70: 500-505 (View)
Broekmans FJ, Kwee J, Hendriks DJ, Mol BW, Lambalk CB (2006). A systematic review of tests predicting ovarian reserve and IVF outcome. Hum Reprod Update; 12:685-718 (View)
ESHRE Capri Workshop Group. Intracytoplasmic sperm injection (ICSI) in 2006 (2007): evidence and evolution. Hum Reprod Update;13:515 – 526 (View)
Fernández A, Castilla JA, Martínez L, Núñez AI, García-Peña ML, Mendoza JL, Blanco M, Maldonado V, Fontes J, Mendoza N (2002). Indicadores de calidad asistencial en un programa de FIV/ICSI. Rev Iberoam Fertil; 19: 249-52 (View)