What is a miscarriage: symptoms, causes and consequences
Spontaneous abortion, also known as miscarriage or spontaneous abortion, is the unintentional loss of a pregnancy before the 20th week of gestation or the loss of a fetus weighing less than 500 grams.
If the gestational loss occurs at later stages, it is not considered a miscarriage, but a premature delivery, although it may also end with the death of the fetus.
The different sections of this article have been assembled into the following table of contents.
Contents
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 7.1.
- 7.2.
- 7.3.
- 7.4.
- 7.5.
- 7.6.
- 7.7.
- 7.8.
- 8.
- 9.
What is miscarriage?
Miscarriage is the involuntary interruption of pregnancy due to the loss of the embryo or fetus before the 20th week of pregnancy.
The loss of a fetus weighing less than 500 grams is also considered a miscarriage.
When the abortion occurs at a more advanced stage of gestation, it is called intrauterine fetal death.
According to statistics, miscarriages occur in the first trimester of pregnancy and, on many occasions, the woman is not even aware that she was pregnant.
Miscarriage is quite common in the population, with 10-20% of pregnancies not reaching full term.
Even so, abortion can have serious consequences for the woman's physical and mental health, as it is a dramatic situation for those who wish to become parents.

A woman's recovery after an abortion usually takes several weeks. Normally, menstruation occurs four to six weeks after the gestational loss has occurred.
The really difficult thing in these cases is to recover emotionally and not go into depression. Miscarriage is a hard blow for the mother-to-be, not only because of the feelings of loss, but also because of the abrupt hormonal changes to which she is subjected in a very short period of time.
There is no need to be afraid or ashamed to ask for help after an abortion. There are support groups and specialized couple's therapies for this type of situation.
Types of miscarriages
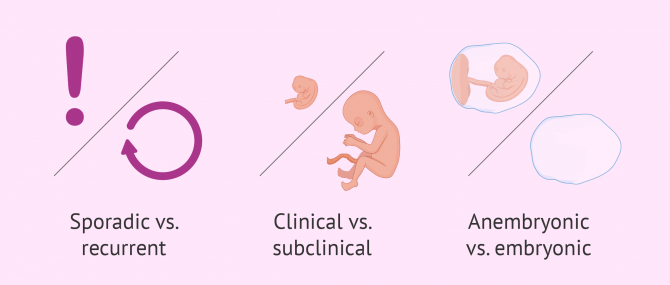
We can distinguish different types of miscarriage depending on the following factors:
- Sporadic vs. recurrent
- depending on whether the miscarriage has occurred on an ad hoc basis or if several miscarriages have taken place. This would be what we call repeat abortion.
- Clinical vs. subclinical
- depending on whether the abortion occurs in advanced stages or if it occurs very early, i.e. close to the time of implantation. The latter is known as biochemical abortion or microabortion and is often confused by women with menstruation.
- Anembryonic vs. embryonic
- in the first case, it is not possible to appreciate the embryo inside the gestational sac by ultrasound, which is known as a hollow egg. In the second case, the embryo is observed but its development has stopped. This type of abortion is also called missed abortion or delayed abortion.
- Complete vs. incomplete
- depending on whether all the uterine contents are removed after the abortion or, on the contrary, there are still fetal remains inside the uterus.

If you want to know more information about the types of abortion, we recommend you to read this article: Types of miscarriage.
Causes
Among the causes that can lead to gestational loss, we find those related to the fetus and those concerning the expectant mother. These are discussed below:
- Fetal causes
- chromosomal defects in the fetus are one of the main reasons why embryonic development may stop.
- Maternal causes
- alterations in the uterine cavity, infections and some autoimmune or endocrine diseases, such as celiac disease or diabetes, are also reasons for fetal loss.

Complications of pregnancy can lead to miscarriage. However, it is true that the severity of these complications increases when there are risk factors such as those detailed below:
- Incorrect or insufficient diet. Nutrition is a factor that must be taken care of during pregnancy.
- When the mother-to-be is a smoker or drinks alcohol.
- If there is any type of hormonal imbalance.
- Having any type of sexually transmitted infection.
- Health problems such as congenital heart disease, kidney disease or thyroid disease.
- Having a high fever.
- Having an IUD in place at the time of conception.
You can obtain more detailed information on this aspect in the following link: Causes of miscarriage.
Symptoms of threatened miscarriage
Although a woman may have certain symptoms or signs of miscarriage, the gestational loss will not always occur. The threat of abortion is simply a warning that this risk exists.
These are the symptoms that may lead you to suspect an imminent miscarriage:
- Heavy vaginal bleeding with clots
- Occurrence of unknown pain or uncommon discomfort of medium-high intensity
- Abdominal pain and severe cramping
- Fever
- Weakness
When a woman presents any sign of threatened miscarriage, she should immediately contact specialists so that a solution can be found in time and the threat does not turn into a miscarriage.
Treatment
In case of threatened abortion, bed rest and uterine sedatives are the most indicated. Progesterone is also given in some cases, although some scientific studies do not agree on its efficiency.
If miscarriage finally occurs, in principle no specific treatment is necessary. Simply put, the fetus and all gestational structures are expelled as blood loss.
If this does not happen, it will be necessary to proceed with evacuation by curettage or uterine curettage.
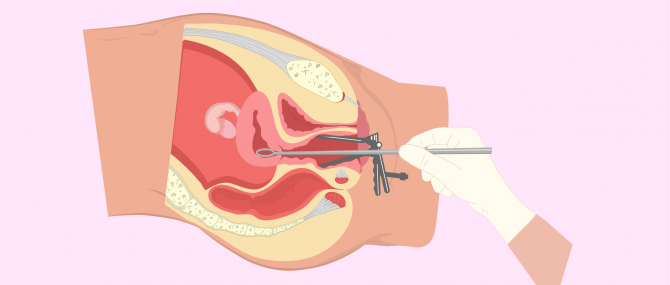
Curettage is performed under anesthesia, dilating the cervix and removing any retained tissue. You can obtain more information here: What is uterine curettage?
There are also cases in which the abortion has just been induced with medications, such as Misoprostol to provoke uterine contractions, which will help eliminate the aborted remains.
This is what is known as pharmacological abortion. However, this method has the disadvantage of having the following side effects:
- Nausea
- Vomiting
- Diarrhea
- Chills
- Headache
- Vaginal bleeding
Finally, the remains of the abortion expelled spontaneously or by scraping the uterine cavity are sent to the laboratory to be studied, to try to diagnose the cause of the abortion and prevent its recurrence.
Assisted procreation, as any other medical treatment, requires that you rely on the professionalism of the doctors and staff of the clinic you choose. Obviously, each clinic is different. Get now your Fertility Report, which will select several clinics for you out of the pool of clinics that meet our strict quality criteria. Moreover, it will offer you a comparison between the fees and conditions each clinic offers in order for you to make a well informed choice.
Prevention of miscarriage
The recommendations to prevent miscarriage or spontaneous abortion are based on respecting the proper care of a pregnant woman.
We have discussed above the most influential risk factors, so if we are seeking to avoid miscarriage, we must also avoid these risks as far as possible.
If the pregnancy is to be premeditated, it is advisable to treat possible diseases or health problems that are related to the abortion or that may be a risk factor.
Hypertension, obesity or diabetes without proper medical control can increase the likelihood of miscarriage. It is also important to analyze whether the mother has had any infection such as toxoplasmosis or rubella, which can cause fetal alterations leading to gestational loss.
Other diseases that should be taken into account when seeking pregnancy, because of their possible relation to miscarriage, are uterine anomalies or immunological diseases.
On the other hand, it is essential to lead a healthy life, with a balanced diet, avoiding excesses and doing moderate exercise. In addition, you should attend all gestational check-ups prescribed by the gynecologist and follow his instructions with discipline.
FAQs from users
If I have had a miscarriage, can it happen again the next time I have a pregnancy?
Approximately one in five pregnancies are terminated in the first trimester and are followed by subsequent normal pregnancies.
In the case of two or more miscarriages, it is advisable to perform a complete study of both members of the couple to diagnose possible causes and prescribe appropriate treatments.
Can stress and anxiety affect pregnancy or lead to miscarriage?
At the level of conception and fertility, stress can cause lack of ovulation during a menstrual cycle and, consequently, decrease the chances of pregnancy. In women with anxiety and high stress levels, ovulation can even decrease by 20%. However, no relationship has been found between stress and miscarriage rate, so stress is ruled out as a cause of miscarriage.
However, there are studies that relate life stress with some effects on pregnancy: there is a very discreet increase in premature births, and in cases of fetal growth retardation in those women with a more stressful rhythm of life. The mechanism by which this happens is still unknown, although these situations must be understood as a sum of factors, in which stress can accentuate a previous predisposition or trigger it, but never be the only responsible, except in very extreme cases.
Pregnancy is a special vital stage and it is advisable to know how to adapt to live this period in a relaxed and healthy way. It is recommended to maintain a certain amount of daily activity and do some type of physical exercise, but in no case is it good to maintain a stressful rhythm of life.
What is a therapeutic abortion?
A therapeutic abortion is a type of abortion that is performed for medical reasons. Common basic medical causes include:
- In case a pregnancy is a life-threatening condition for the mother.
- To protect the physical and/or mental health of the mother.
- When there exists risk of birth defects or genetic disease.
- In multiple pregnancies, it is possible to perform a selective reduction or multifetal pregnancy reduction (MFPR) to a number of fetuses that removes serious risks and makes the pregnancy a viable one.
- When there is a serious risk for the life of the developing baby, either because there exists a malformation, or because there is a high risk of being born dead (stillbirth) or death right after being born
What is a delayed abortion?
We speak of delayed abortion or missed abortion when the woman, despite the fact that the embryo has already stopped its development, does not manage to expel the gestational sac until a few weeks or even months have passed.
Is curettage necessary in case of incomplete abortion?
Yes, it is generally recommended to wash the abortive remains if they have not been completely expelled.
Curettage allows for the removal of any remaining fetal tissue, thus avoiding possible infections.
What is a septic abortion?
We speak of septic or infected abortion when the lining of the uterus or any remaining products of conception become infected. It can occur if parts of the fetal or placental tissue remain in the uterus after an incomplete abortion.
Is it possible to have a miscarriage of a twin?
Yes, this can happen during a multiple pregnancy and is what is known as vanishing twin syndrome.
When doing an ultrasound, it is observed that one of the fetuses is smaller, does not have a heartbeat or has already disappeared. What happens is that this fetus stops its development at an early stage and is reabsorbed by the tissues of the uterus without causing complications.
The other baby continues to develop normally and does not need to take any risks.
I want to get pregnant fast after a miscarriage, is it possible?
Although the WHO recommends waiting about six months to seek pregnancy again, there are numerous studies that indicate that the sooner the pregnancy is resumed, the lower the chances of suffering a new miscarriage or other gestational complications.
The WHO recommendations are based fundamentally on emotional aspects, since miscarriage is a hard trauma and it is convenient to have overcome this grief and be prepared to face the new pregnancy with illusion. On the other hand, the studies that indicate that it is not necessary to wait to conceive again after the abortion are based on physiological aspects of the female body.
In any case, it is important to consult your doctor. Many specialists recommend waiting an average of two menstrual periods before trying again. However, this depends very much on the type of miscarriage that has occurred and the consequences of the miscarriage both physically and emotionally.
Recommended readings
Despite the belief of many people, miscarriages do not affect female fertility. A woman can safely become pregnant again after an abortion unless there are complications. You can read more about this topic in the following post: Fertility after miscarriage.
On the other hand, there are discrepancies about the recommended waiting time for attempting a new pregnancy after miscarriage. You will find all the information on this subject in the following article: How long does it take after an abortion to try to get pregnant?
We make a great effort to provide you with the highest quality information.
🙏 Please share this article if you liked it. 💜💜 You help us continue!
References
Chung et al. Spontaneous abortion: a randomized, controlled trial comparing surgical management with conservative management using misoprostol; Fertility and Sterility 1999; 71:1054 – 9.
De la Fuente, P. (1997). Aborto espontáneo. En: Fabre E, editor. Manual de asistencia a la patología obstétrica. Sociedad Española de Ginecología y Obstetricia. Sección de Medicina Perinatal. 1ª Ed. Zaragoza: INO; pp. 71-87
Levy T, Dicker D, Ashkenazi J, Feldberg D, Shelef M, Goldman JA. The prognostic value and significance of preclinical abortions in in vitro fertilization-embryo transfer programs. Fertil Steril 1991;56:71–4.
Luise et al. Outcome of expectant management of spontaneous first trimester miscarriage: observational study; British Medical Journal 13 April 2002 pp 873 - 875.
Nielsen and Hahlin. Expectant management of first-trimester spontaneous abortion; Lancet 1995;345: 84 – 86.
Verdú LI, Santamaría R. (2003). Aborto: concepto y clasificación. Etiología, anatomía patológica clínica y tratamiento. En: Cabero L. editor. Tratado de Obstetricia, Ginecología y Medicina de la Reproducción. 1ª Ed. Madrid: Editorial Médica Panamericana; pp. 500-508
Wang JX, Norman RJ,Wilcox AL. Incidence of spontaneous abortion among pregnancies produced by assisted reproductive technology. Hum Reprod 2004;19:272 – 227.
Wilcox AJ, Weinberg CR, O’Connor JF, Baird DD, Schlatterer JP, Canfield RE, Armstrong EG, Nisula BC. Incidence of early loss of pregnancy. N Engl J Med 1988;319:189 – 194.
Zinaman MJ, O’Conner J, Clegg ED, Brown CC, Selevan SG. Estimates of human fertility and pregnancy loss. Fertil Steril 1996;65:503– 509.