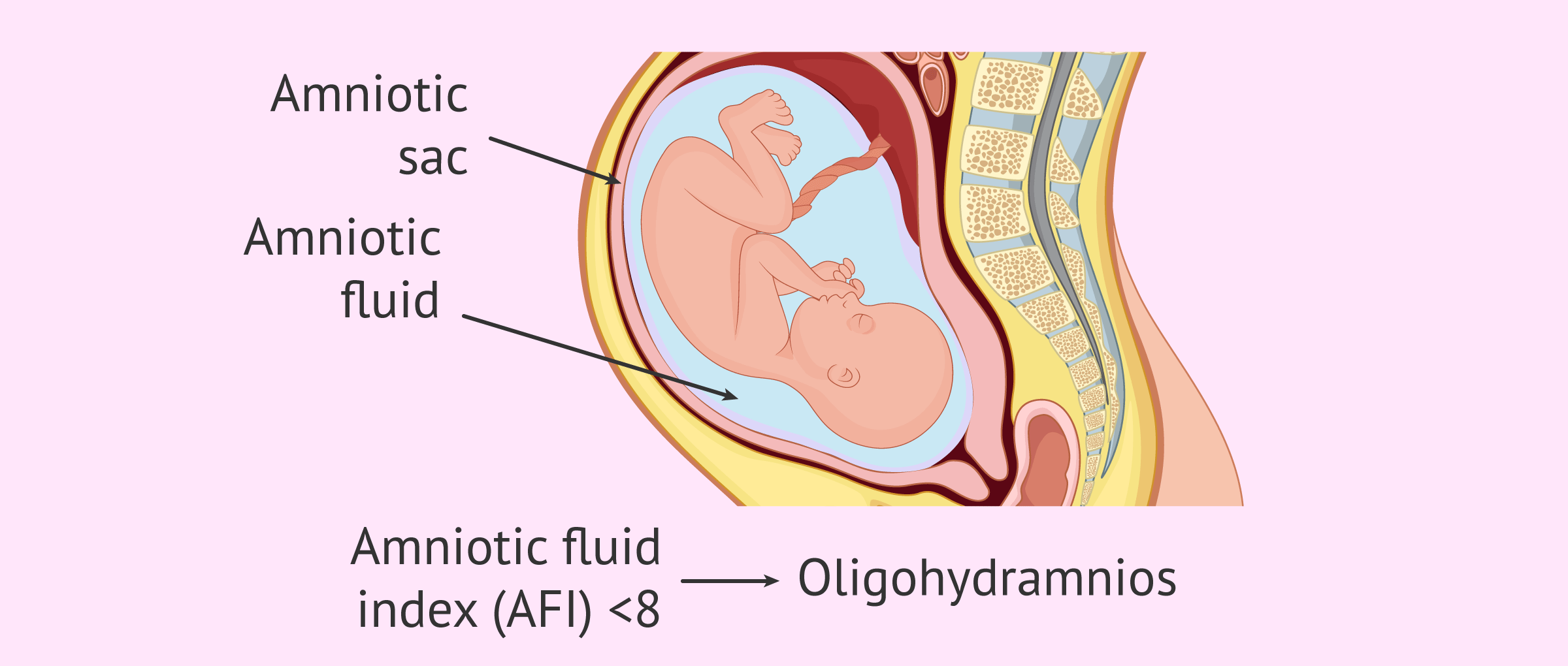
Amniotic fluid is the fluid that surrounds the fetus during gestation. It is located inside the amniotic sac and has the function of protecting the fetus throughout its development, from the beginning of pregnancy until the birth of the baby.
An abnormal amount of amniotic fluid is indicative of fetal abnormalities or problems in the mother that may jeopardize the pregnancy. Therefore, it is important to measure the volume of amniotic fluid in ultrasound scans, especially in the last trimester.
A small amount of amniotic fluid is referred to as oligohydramnios while an excessive amount of amniotic fluid is referred to as polyhydramnios.
Provided below is an index with the 8 points we are going to expand on in this article.
- 1.
- 1.1.
- 2.
- 3.
- 4.
- 5.
- 5.1.
- 5.2.
- 5.3.
- 5.4.
- 6.
- 7.
- 8.
Definition of oligohydramnios
The term oligohydramnios refers to the small amount of amniotic fluid in pregnancy. This disorder affects less than 10% of pregnant women, although only about 5% are diagnosed.
Oligohydramnios usually occurs in the last trimester, especially if the pregnant woman is past her due date, although it can also occur at any other time during pregnancy.
In general, the consequences of oligohydramnios are more severe if it appears in the first two trimesters of gestation than in the third trimester. Despite this, most pregnancies with oligohydramnios manage to develop normally and result in the birth of healthy babies.
The amount of amniotic fluid varies throughout gestation. On average, the amniotic sac contains about 30 ml of fluid at 10 weeks, 100 ml at week 14, 200 ml at week 16, and reaches its maximum at week 34, with about 800 ml of amniotic fluid.
After 36 weeks, the amount of amniotic fluid gradually decreases to 600 ml at the end of pregnancy, but it should never disappear.
How is amniotic fluid measured?
The amount of amniotic fluid can be measured with an ultrasound scan using the so-called Phelan's method or, in other words, by calculating the amniotic fluid index (AFI).
This method consists of dividing the uterine cavity into four quadrants and then measuring the diameters of the maximum amniotic fluid-free lacunae in each quadrant.
The AFI is obtained by adding these 4 measurements. The normal AFI value should be between 8-24 cm to consider that the amniotic fluid volume is correct.
An AFI<8 or an amniotic fluid volume of less than 500 ml between 32 and 36 weeks of gestation are indicative of oligohydramnios.
Causes
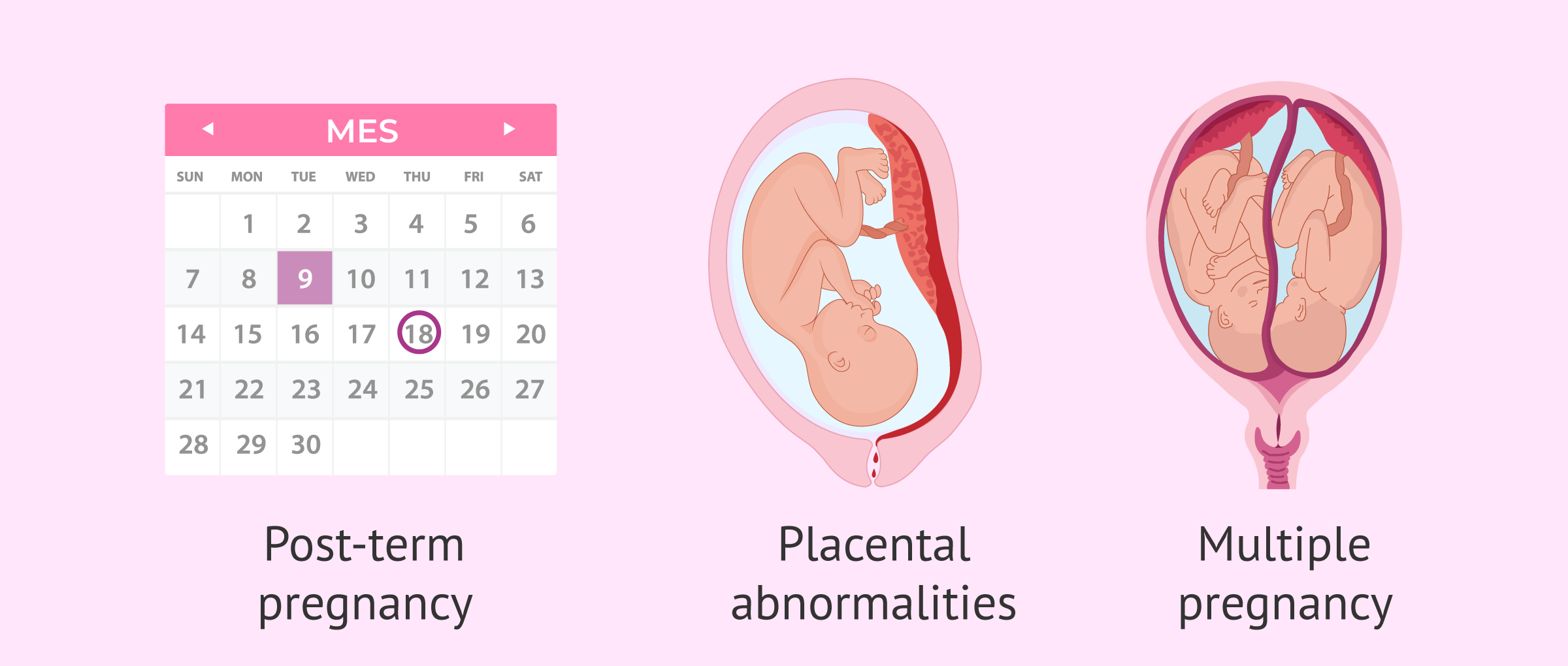
It is not always possible to find out for sure what the exact cause of oligohydramnios is. However, the main reasons for decreased amniotic fluid are as follows:
- Post-term pregnancy
- when the pregnancy is about two weeks beyond the approximate due date.
- Premature rupture of membranes (PROM)
- the amniotic sac ruptures before delivery and some of the amniotic fluid may escape. The woman may notice these losses in her previous clothes.
- Alterations in the placenta
- such as placental abruption, which can prevent sufficient blood and nutrients from reaching the fetus and stop the fetus from producing urine.
- Maternal problems
- preeclampsia, chronic hypertension, dehydration, diabetes, lupus, etc.
- Multiple pregnancy
- the occurrence of intergemellar transfusion syndrome, in which one of the twins has too little amniotic fluid while the other generates too much.
- Fetal alterations
- congenital malformations affecting the kidneys and urinary tract, fetal growth restriction, fetal death, etc.
- Medications
- drugs containing angiotensin-converting enzyme inhibitors, such as captopril to treat hypertension, can cause oligohydramnios.
Symptoms and complications
Insufficient amniotic fluid can cause more or less serious problems for the baby depending on the stage of pregnancy.
In most cases, oligohydramnios does not cause any symptoms in the woman and, therefore, will only be diagnosed in a control ultrasound. The only possible symptom is loss of amniotic fluid if there is a rupture of the membrane.
We will now discuss the possible risks of oligohydramnios in each trimester of pregnancy:
- First trimester
- lack of amniotic fluid in early pregnancy can have fatal consequences since this is when all the organs of the future baby are formed. Thus, oligohydramnios can lead to malformations of the lungs, arms, or legs. It also poses a risk of miscarriage, premature delivery or intrauterine fetal death.
- Second trimester
- during this period, oligohydramnios affects fetal growth and may also impede the proper formation and maturation of the lungs.
- Third trimester
- although complications are minor, the lack of amniotic fluid in late pregnancy increases the risk of umbilical cord compression, which affects the baby's oxygenation and heart rate. Oligohydramnios also increases the risk of complications during labor, leading to the need for a cesarean section.
Treatment
The treatment of oligohydramnios consists of a more exhaustive control of the pregnancy. The woman will have to have several ultrasounds to make sure that the fetus is growing at the right rate.
Other indications to treat the lack of amniotic fluid are to drink a lot, control the baby's kicking and activity, partial or complete rest, etc. This will depend on how far along the pregnancy is and whether there are other associated disorders.

If the woman is at an advanced stage of gestation, it is very likely that labor will be induced, especially if fetal distress is confirmed.
A novel technique that can help maintain amniotic fluid levels during labor is amnio-infusion. It consists of inserting a catheter through the cervix and constantly pumping a saline solution into the amniotic sac. This reduces the risk of umbilical cord compression and increases the likelihood of a natural delivery.
FAQs from users
What recommendations should a woman with oligohydramnios follow?
Oligohydramnios occurs when the volume of amniotic fluid is decreased during gestation. The diagnosis is ultrasound, measuring the amount of amniotic fluid by ultrasound.
We can divide the causes of Oligohydramnios into three main groups:
- Fetal causes: restricted intrauterine growth (RIC), chronologically prolonged gestation (CPG), fetal infection or alterations of the fetal urinary tract.
- Placental-membrane causes: premature rupture of membranes (PROM) accounts for most cases.
- Maternal causes: maternal medication.
Depending on the cause of Oligohydramnios and the time of pregnancy, your obstetrician will give you recommendations.
What is the reason for the low amount of amniotic fluid?
There are several causes of amniotic fluid shortage in pregnancy, such as rupture of the membranes, placental abruption, hypertension, fetal malformations, prolonged pregnancy, etc.
How can oligohydramnios be classified?
The classification of oligohydramnios based on its severity is as follows:
- Mild
- AFI between 6 and 7.
- Moderate
- API between 4 and 5.
- Severe
- ILA<3.
It should be noted that there are variations in this classification depending on the specialist. In addition, it is also necessary to assess other parameters, such as blood pressure, to make an accurate diagnosis of oligohydramnios.
What are the consequences of moderate or severe oligohydramnios?
The lack of amniotic fluid for a prolonged period of time can affect the organogenesis and growth of the fetus, especially the maturation of the lungs, leading to pulmonary hypoplasia.
At the time of delivery, oligohydramnios can also lead to complications such as fetal distress or meconium aspiration syndrome (MAS), leading to emergency cesarean section.
Recommended readings
One of the causes of oligohydramnios is the rupture of the amniotic sac before delivery. If you want to know all the details about this, we recommend you to read the following article: How do I know if I am losing amniotic fluid in pregnancy?
Another alteration in the amount of amniotic fluid is polyhydramnios, that is, excess amniotic fluid. If you want to know what this alteration consists of, you can continue reading here: What is polyhydramnios?
We make a great effort to provide you with the highest quality information.
🙏 Please share this article if you liked it. 💜💜 You help us continue!
References
Authors and contributors



More information about Cristina Algarra Goosman

Hi, I am 32 weeks pregnant and during the last few days I have felt like I am getting very wet, I thought it was urine but is it possible that it is amniotic fluid? I’m a little worried, I’m not having contractions and I don’t notice anything strange. Thank you
Hello Norma,
During the last trimester, amniotic fluid leakage is possible for several reasons, although it is usually due to premature rupture of the membranes.
I recommend that you see your doctor so that he/she can evaluate if the fluid is indeed amniotic fluid and if the amount inside your uterus has decreased.
It is important to determine this as soon as possible because excessive fluid loss can cause problems with the umbilical cord and therefore the baby’s well-being.
I hope I have helped you,
Best regards.
Amniotic fluid is what is known as water breaking, isn’t it? What is its function?
Hi Kimberly,
Indeed, this is the liquid that upon release is known as “breaking your water”. The amniotic fluid is responsible for protecting the baby, cushioning the baby’s movements, and helping with lung development.
Depending on what trimester you are in and the amount of amniotic fluid inside the amniotic sac will mean normal values or some potentially dangerous alteration for the fetus.
I recommend that you read the following article where it explains both its characteristics and functions: What is amniotic fluid?
I hope I have helped you.
Best regards