What Is a Testicular Biopsy? – Purpose & Procedure
A testicular biopsy consists of a small surgery that allows the extraction of tissue from the testicles and its observation under a microscope.
It can be done by opening the skin of the scrotum or by a puncture and aspiration with a special needle. A local or general anesthetic is administered in the area, so the testicular biopsy is painless.
In general, this technique is performed with two objectives: diagnostic and therapeutic. Thus, testicular biopsy allows determining the cause of male sterility and sperm collection when a seminogram shows azoospermia (absence of sperm in the ejaculated semen).
Usually, a testicular biopsy does not cause serious complications. The most common risks include wound infection or minor discomfort in the hours following the operation.
The different sections of this article have been assembled into the following table of contents.
Contents
- 1.
- 1.1.
- 2.
- 3.
- 4.
- 4.1.
- 4.2.
- 5.
- 6.
- 7.
- 7.1.
- 7.2.
- 7.3.
- 7.4.
- 7.5.
- 7.6.
- 7.7.
- 8.
What does it consist of?
Testicular biopsy is a superficial surgical procedure based on the removal of one or more portions of tissue through small incisions in the testicles. These incisions are sutured with stitches that fall out or are reabsorbed.
The portions of the tissue are then looked at under a microscope to detect the presence or absence of sperm. Thus, the tissue of the testicles can also be studied.
The procedure for obtaining sperm in the laboratory is very delicate. In the seminiferous tubules (tubes inside the testicle) there are spermatozoa, but also other types of cells that can make it difficult to visualize them. Therefore, this surgical test is performed by a specialist physician (urologist) supported by a biologist.


In general, it is a simple and painless technique because it is performed under anesthesia.
40% of sterility cases in couples are of male origin, either because of alterations in the quality of the semen or because of ejaculation problems.
Testicular biopsy is a relatively modern procedure that allows couples to achieve a pregnancy through IVF treatment with intracytoplasmic sperm injection (ICSI), without the need for donor sperm.
Objective of testicular biopsy
Thanks to this surgery, it is possible to determine whether spermatogenesis (sperm production) occurs normally in the testicle.
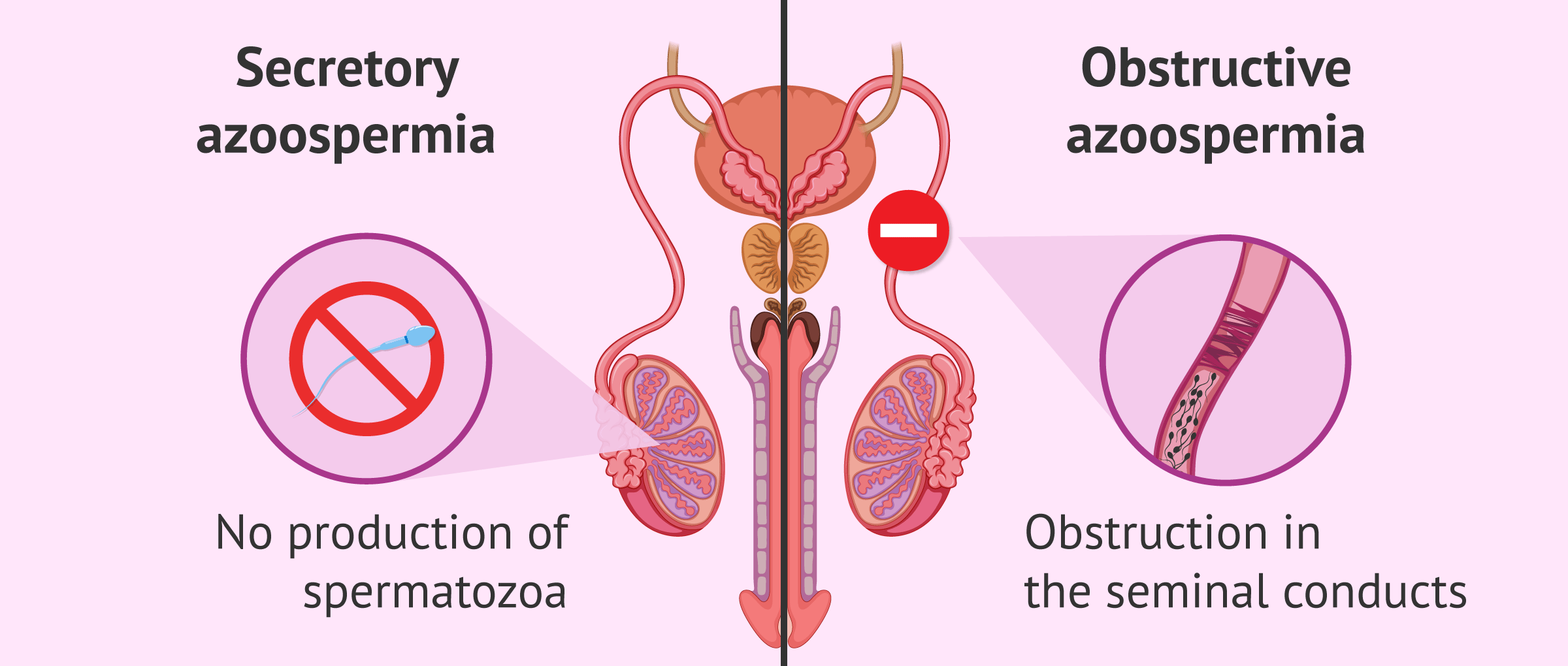
Therefore, testicular biopsy allows us to distinguish between a pathology:
- of obstructive type: if the seminal ducts that allow the semen to exit are blocked. This type of pathology is known as obstructive azoospermia.
- of secretory type: the production of spermatozoa does not exist or the spermatozoa do not finish their maturation process. That refers to the secretory azoospermia.
This diagnostic purpose allows us to say what kind of problem the patient is suffering from and to evaluate the origin of male infertility. Thus, the specialist proposes the most appropriate treatment.
Another objective of this test is the spermatozoa retrieval directly from the testicle. This is done when no sperm are found in the ejaculate. In this way, sperm are obtained to be frozen and/or used fresh later in an ICSI fertility treatment.
It should be noted that only as many sperm as eggs are needed for ICSI. For this reason, this technique can be performed with poor quality seminal samples or samples recovered from the testicle.
Assisted procreation, as any other medical treatment, requires that you rely on the professionalism of the doctors and staff of the clinic you choose. Obviously, each clinic is different. Get now your Fertility Report, which will select several clinics for you out of the pool of clinics that meet our strict quality criteria. Moreover, it will offer you a comparison between the fees and conditions each clinic offers in order for you to make a well informed choice.
Indications of testicular biopsy
Testicular biopsy is usually done to find the cause of male infertility when a seminogram shows abnormal results. This technique is recommended in cases of azoospermia, oligospermia, and severe alterations of seminal quality.
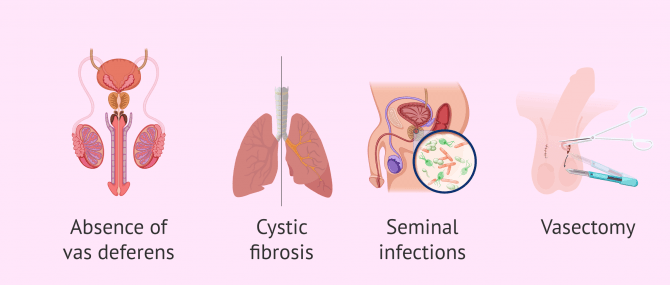
It is also indicated in cases of obstruction of the seminal duct, which have different causes:
- Absence of vas deferens.
- Cystic Fibrosis.
- Infections.
- Vasectomy.

On the other hand, a testicular biopsy can be performed in the presence of a tumor to determine its status.
Testicular biopsy should not be performed when the absence of sperm is caused by hormonal disorders or there is clear evidence of their absence in the testicles.
Types of testicular biopsies
The method of biopsy to be performed will depend on the reason for the exam. Your doctor will discuss your options.
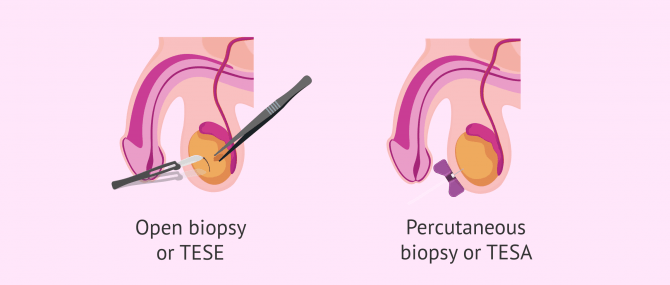
In general, there are two techniques for obtaining sperm from the testicle:
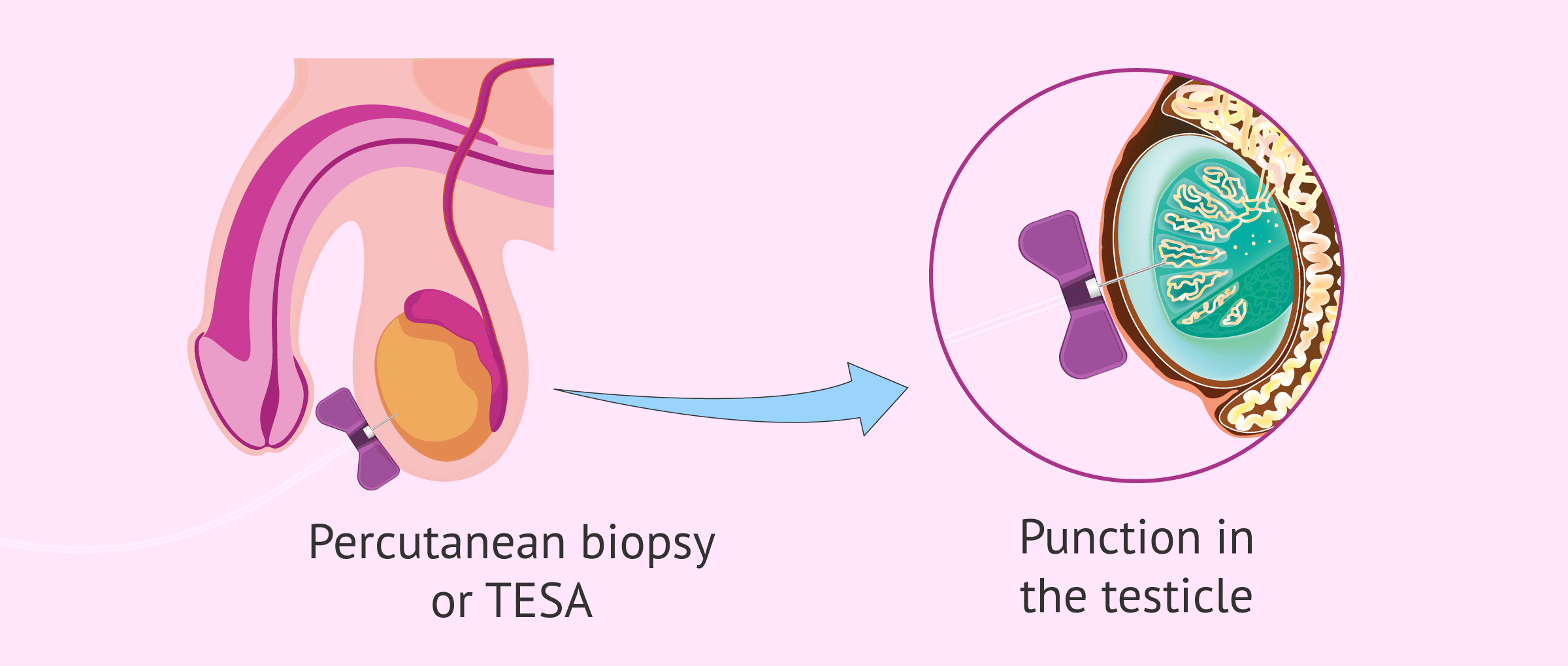
- Testicular sperm extraction (TESE), also called open biopsy, is the biopsy itself. Although TESE is indicated in patients with obstructive azoospermia, it is also applied in some situations of secretory azoospermia.
- Testicular sperm aspiration (TESA): also known as percutaneous biopsy. This method is less invasive than TESE and is useful for men who have sterility problems caused by a blockage in sperm ejaculation.
The aim of both procedures is to obtain spermatozoa for subsequent use in in vitro fertilisation (IVF) treatment. Although they have the same purpose, the decision to apply one method or the other will depend on the patient's particular situation.
It is recommended that sexual activity be avoided for 1-2 weeks after the testicular biopsy.
Procedure
Testicular biopsy does not require hospital admission since it is a simple technique. However, it is an unpleasant test for the man compared to a seminogram or blood test.
Depending on the type of testicular biopsy to be performed (TESE or TESA), the method performed is different.
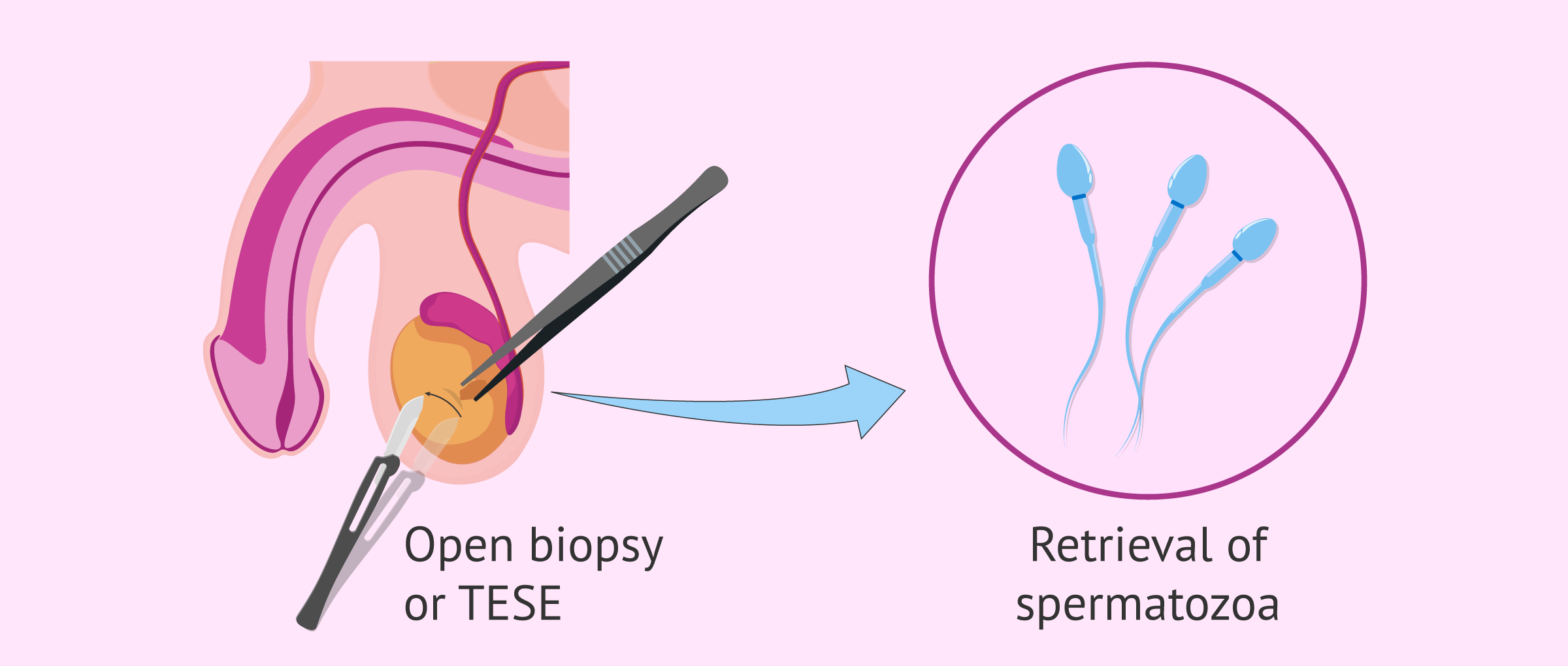
Open testicular biopsy or TESE
The surgical procedure of an open biopsy is performed under local anesthesia and sometimes combined with sedation. The duration of the procedure is approximately 15 to 20 minutes.
The process consists of removing small fragments of the testicle to be evaluated under a microscope to look for sperm. To do this, a small incision of 2-3 cm is made in the skin of the scrotum and another in the testicle. In the end, stitches are placed to close the wound and it is covered with a simple dressing. The technique is repeated on the other testicle if necessary.
The removed tissue is fractionated in the laboratory and observed under the microscope. In this way, part of the tissue is used for the recovery of viable sperm, and another part is used to establish a diagnosis of the cause of infertility.
Once the sperm are obtained, they can be frozen in liquid nitrogen at -196ºC or used directly to fertilize the woman's eggs extracted by ovarian puncture during an IVF treatment.
Percutaneous testicular biopsy or TESA
This model of testicular biopsy consists of making a puncture in the testicle with the help of a special needle attached to a syringe. This is a less aggressive methodology compared to open biopsy.
However, TESA also has several disadvantages over TESE:
- Few sperm may be obtained and the patient may have to undergo another open testicular biopsy.
- Increased likelihood of complications and side effects.
Therefore, a percutaneous biopsy is not frequently used for sperm aspiration. In these cases, sperm aspiration is usually used in the epididymis.
Complementary studies
Once the testicular tissue is obtained, two types of complementary studies can be performed:
- Histology study: is performed when the seminogram shows a concentration of spermatozoa below the limits of normality (oligozoospermia) or if there are no spermatozoa in the ejaculate (azoospermia). Here the testicular tissue and its ability to produce sperm are analyzed, as well as finding out at what point in the spermatogenesis this production is interrupted.
- Meiosis or cytogenetic study: evaluates the structure, composition and chromosome arrangement at the different stages of sperm formation. This test is performed when there are previous repeated miscarriages or low sperm mobility (asthenozoospermia). The use of a testicular biopsy for a meiotic study is quite controversial since there are no clear parameters for this analysis.
Complications and risks of testicular biopsy
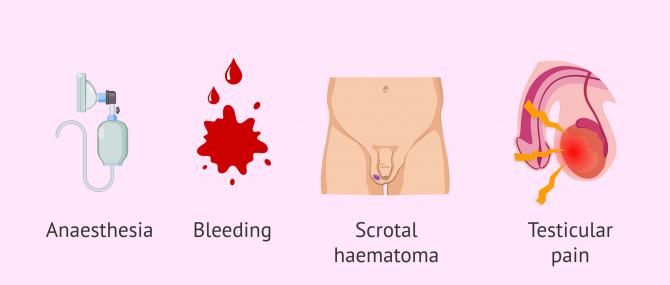
Complications and risks associated with testicular biopsy are rare. However, since it is a surgical procedure, complications may arise from the anesthesia. In any case, these complications will be referred to as the treatment that the specialist doctor decides.
Other side effects of testicular biopsy, although uncommon, are the following:
- Bleedings.
- Wound infection.
- Bruise on the skin of the scrotum.
- Intratesticular hematoma accompanied by persistent pain of the testicles. This bruise is usually reabsorbed within a few weeks.
- Swelling of the testicle that stops with the administration of analgesics and anti-inflammatories.
On the other hand, the assisted reproduction treatment can also be canceled if no sperm are recovered in the biopsy. In this situation, the eggs retrieved in the woman's follicular puncture would be frozen, while waiting to decide whether to repeat the biopsy or opt for donor sperm.
Waiting for the results of the biopsy may create a situation of anxiety in the couple. For this reason, specialists advice to seek psychological support.
FAQs from users
Can sexual intercourse take place before testicular biopsy?
Testicular biopsy is used to obtain sperm when sperm cannot be obtained by ejaculation. It is indicated in cases of azoospermia, when sperm have been obtained without sperm in the semen sample or to achieve pregnancy after a vasectomy.
In cases of azoospermia, sperm will be retrieved if the cause is an obstruction (obstructive azoospermia). In case the problem is in sperm production, if a sperm-producing focus of the testicle is not located, it is very difficult to find sperm in the biopsy as well.
Since the seminal sample does not contain sperm (which is the reason why biopsy is usually indicated), having sexual intercourse before the biopsy will not influence the results of the procedure.
How many sperm need to be obtained in a testicular biopsy?
Firstly, it is necessary to define very well what these spermatozoa obtained from the testicle are going to be used for and what type of azoospermia we are talking about.
In cases of secretory azoospermia, as it is more difficult to obtain sperm, microinjection can be attempted even if the number is very low, always informing the patients of the prognosis. There is no defined minimum number of sperm but there must be at least two or three times the number of oocytes to be microinjected to ensure a certain margin of safety. Normally, freezing samples in these cases is very difficult due to the shortage.
In contrast, in obstructive azoospermia, the scenario is usually different. Embryologists assess that the concentration of sperm present is as before, 2-3 times more than the number of oocytes to be microinjected, and if the sample has a higher concentration it can be frozen for future use. As long as the sample can be frozen, it will be the most convenient to avoid future surgeries if the in vitro fertilization treatment fails.
Read more
Does a testicular biopsy hurt?
No. Open testicular biopsy or TESE can be performed under local or general anesthesia. The most common method is to sedate the patient, so he or she will not notice anything.
In percutaneous biopsy or TESA, local anesthesia is usually used, so the patient may feel some pressure but no pain.
Is sexual intercourse possible after a testicular biopsy?
A period of sexual abstinence of 1 to 2 weeks is recommended. After this time, the patient can return to normal sexual activity.
Can sperm obtained from a testicular biopsy be used to perform artificial insemination?
No. The amount of sperm obtained in a testicular biopsy is very small, so artificial insemination is not possible.
In these cases, the recommended technique is ICSI.
How much does a testicular biopsy cost?
The price of a testicular biopsy ranges from approximately 2,500-6,000 dollars, depending on the center where it is performed and the method used.
Does a testicular biopsy always yield spermatozoa?
No. The probability of finding spermatozoa with a testicular biopsy is high, but it is not 100%. The cause of the absence of sperm in the ejaculate is important to predict the probability of success of the technique.
Suggested for you
If you wish to obtain information about the normal values of a seminogram in man, I encourage you to click on the following link: Sperm Test Results Explained- Interpretation & Normal Values.
Azoospermia is one of the leading causes of testicular biopsy. Therefore, I invite you to continue reading this article: Azoospermia- Can a Man Actually Have Zero Sperm Count?
We make a great effort to provide you with the highest quality information.
🙏 Please share this article if you liked it. 💜💜 You help us continue!